

Lack of evidence of increased mortality among patients with atrial fibrillation taking digoxin: findings from post hoc propensity-matched analysis of the AFFIRM trial
- PMID: 23592708
- PMCID: PMC3659306
- DOI: 10.1093/eurheartj/eht120
Lack of evidence of increased mortality among patients with atrial fibrillation taking digoxin: findings from post hoc propensity-matched analysis of the AFFIRM trial
Abstract
Aims: Digoxin is recommended for long-term rate control in paroxysmal, persistent, and permanent atrial fibrillation (AF). While some analyses suggest an association of digoxin with a higher mortality in AF, the intrinsic nature of this association has not been examined in propensity-matched cohorts, which is the objective of the current study.
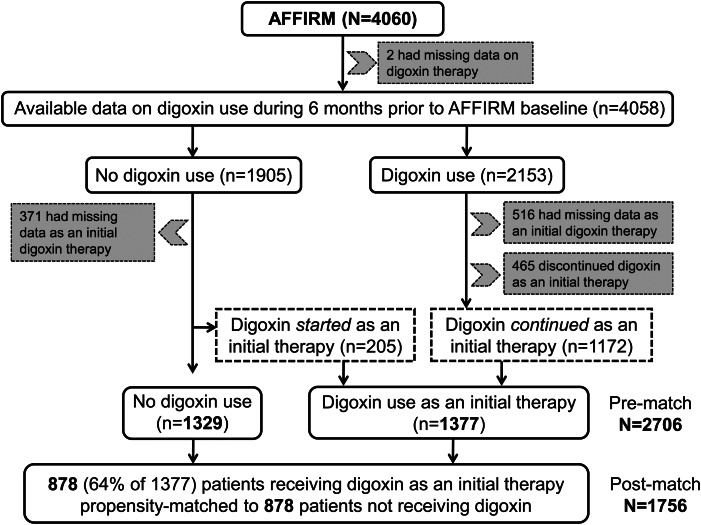
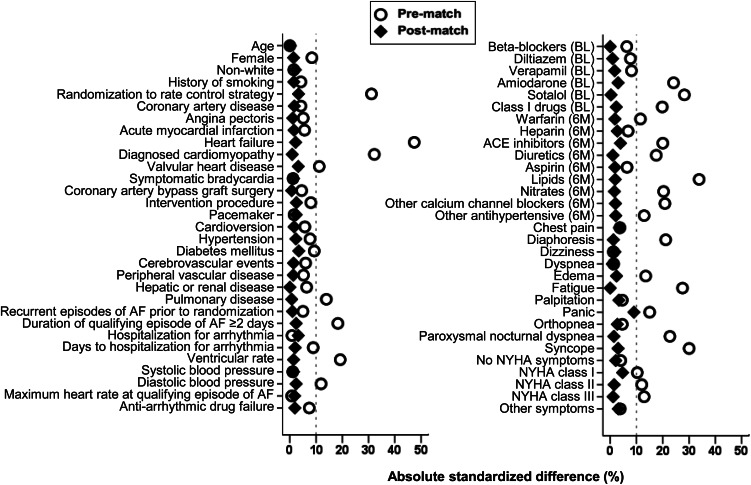
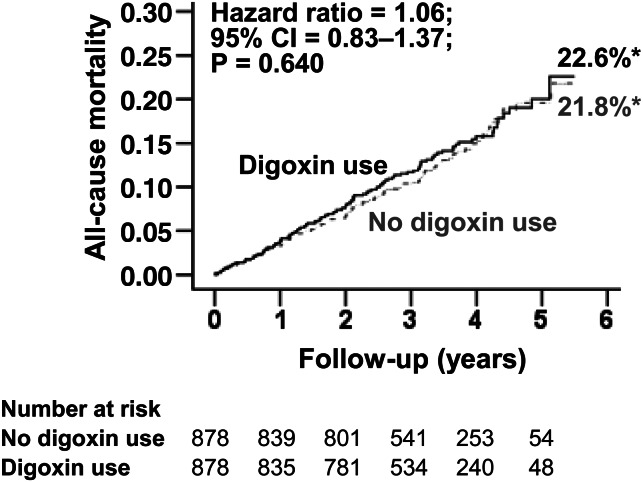
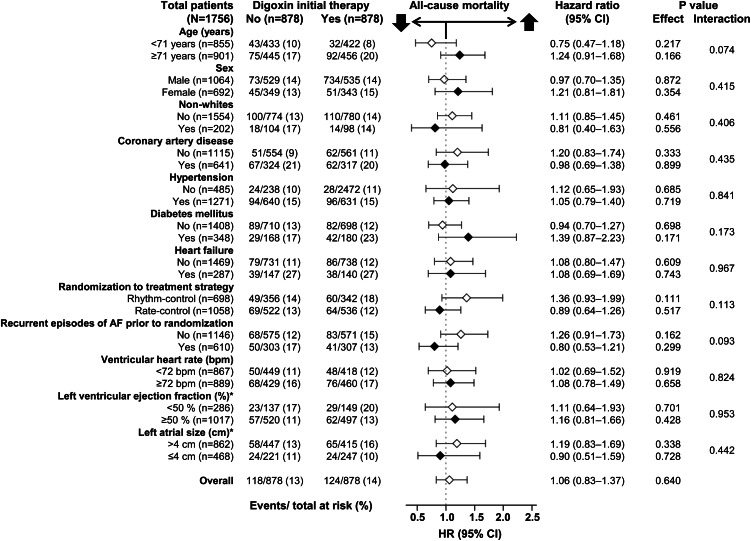
Methods and results: In Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM), 4060 patients with paroxysmal and persistent AF were randomized to rate (n = 2027) vs. rhythm (n = 2033) control strategies. Of these, 1377 received digoxin as initial therapy and 1329 received no digoxin at baseline. Propensity scores for digoxin use were estimated for each of these 2706 patients and used to assemble a cohort of 878 pairs of patients receiving and not receiving digoxin, who were balanced on 59 baseline characteristics. Matched patients had a mean age of 70 years, 40% were women, and 11% non-white. During the 3.4 years of the mean follow-up, all-cause mortality occurred in 14 and 13% of matched patients receiving and not receiving digoxin, respectively [hazard ratio (HR) associated with digoxin use: 1.06; 95% confidence interval (CI): 0.83-1.37; P = 0.640]. Among matched patients, digoxin had no association with all-cause hospitalization (HR: 0.96; 95% CI: 0.85-1.09; P = 0.510) or incident non-fatal cardiac arrhythmias (HR: 0.90; 95% CI: 0.37-2.23; P = 0.827). Digoxin had no multivariable-adjusted or propensity score-adjusted associations with these outcomes in the pre-match cohort.
Conclusions: In patients with paroxysmal and persistent AF, we found no evidence of increased mortality or hospitalization in those taking digoxin as baseline initial therapy.
Keywords: Atrial fibrillation; Digoxin; Hospitalization; Mortality; Propensity score.
Figures
Comment in
-
Digoxin for patients with atrial fibrillation and heart failure: paradise lost or not?Eur Heart J. 2013 May;34(20):1468-70. doi: 10.1093/eurheartj/ehs483. Epub 2013 Jan 16. Eur Heart J. 2013. PMID: 23324547 No abstract available.
-
When 'digoxin use' is not the same as 'digoxin use': lessons from the AFFIRM trial.Eur Heart J. 2013 May;34(20):1465-7. doi: 10.1093/eurheartj/eht087. Epub 2013 Apr 16. Eur Heart J. 2013. PMID: 23592709 No abstract available.
References
-
- Feinberg WM, Blackshear JL, Laupacis A, Kronmal R, Hart RG. Prevalence, age distribution, and gender of patients with atrial fibrillation. Analysis and implications. Arch Intern Med. 1995;155:469–473. - PubMed
-
- Camm AJ, Kirchhof P, Lip GY, Schotten U, Savelieva I, Ernst S, Van Gelder IC, Al-Attar N, Hindricks G, Prendergast B, Heidbuchel H, Alfieri O, Angelini A, Atar D, Colonna P, De Caterina R, De Sutter J, Goette A, Gorenek B, Heldal M, Hohloser SH, Kolh P, Le Heuzey JY, Ponikowski P, Rutten FH European Heart Rhythm A, European Association for Cardio-Thoracic S. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Eur Heart J. 2010;31:2369–2429. - PubMed
-
- Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, Schron EB, Kellen JC, Greene HL, Mickel MC, Dalquist JE, Corley SD The AFFIRM Investigators. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002;347:1825–1833. - PubMed
-
- Corley SD, Epstein AE, DiMarco JP, Domanski MJ, Geller N, Greene HL, Josephson RA, Kellen JC, Klein RC, Krahn AD, Mickel M, Mitchell LB, Nelson JD, Rosenberg Y, Schron E, Shemanski L, Waldo AL, Wyse DG Investigators A. Relationships between sinus rhythm, treatment, and survival in the Atrial Fibrillation Follow-Up Investigation of Rhythm Management (AFFIRM) Study. Circulation. 2004;109:1509–1513. - PubMed
-
- Whitbeck MG, Charnigo RJ, Khairy P, Ziada K, Bailey AL, Zegarra MM, Shah J, Morales G, Macaulay T, Sorrell VL, Campbell CL, Gurley J, Anaya P, Nasr H, Bai R, Di Biase L, Booth DC, Jondeau G, Natale A, Roy D, Smyth S, Moliterno DJ, Elayi CS. Increased mortality among patients taking digoxin analysis from the AFFIRM study. Eur Heart J. Advance Access published November 27, 2012 doi:10.1093/eurheartj/ehs348. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
