

TBX4 mutations (small patella syndrome) are associated with childhood-onset pulmonary arterial hypertension
- PMID: 23592887
- PMCID: PMC3717587
- DOI: 10.1136/jmedgenet-2012-101152
TBX4 mutations (small patella syndrome) are associated with childhood-onset pulmonary arterial hypertension
Abstract
Background: Childhood-onset pulmonary arterial hypertension (PAH) is rare and differs from adult-onset disease in clinical presentation, with often unexplained mental retardation and dysmorphic features (MR/DF). Mutations in the major PAH gene, BMPR2, were reported to cause PAH in only 10-16% of childhood-onset patients. We aimed to identify more genes associated with childhood-onset PAH.
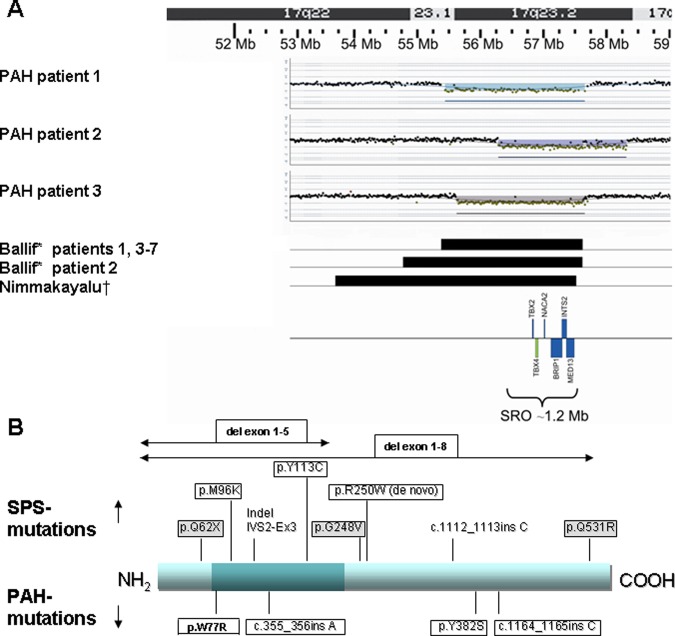
Methods: We studied 20 consecutive cases with idiopathic or heritable PAH. In patients with accompanying MR/DF (n=6) array-comparative genomic hybridisation analysis was performed, with the aim of finding common deletion regions containing candidate genes for PAH. Three patients had overlapping deletions of 17q23.2. TBX2 and TBX4 were selected from this area as candidate genes and sequenced in all 20 children. After identifying TBX4 mutations in these children, we subsequently sequenced TBX4 in a cohort of 49 adults with PAH. Because TBX4 mutations are known to cause small patella syndrome (SPS), all patients with newly detected TBX4 mutations were screened for features of SPS. We also screened a third cohort of 23 patients with SPS for PAH.
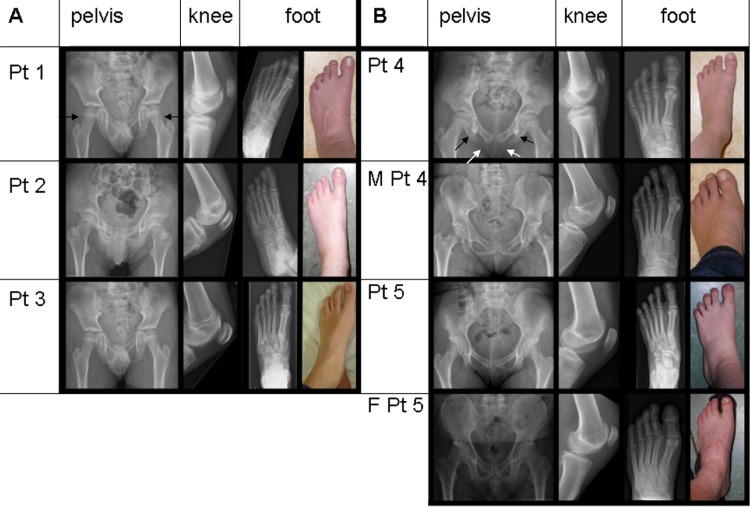
Results: TBX4 mutations (n=3) or TBX4-containing deletions (n=3) were detected in 6 out of 20 children with PAH (30%). All living patients and two parents with TBX4 mutations appeared to have previously unrecognised SPS. In the adult PAH-cohort, one TBX4 mutation (2%) was detected. Screening in the cohort of (predominantly adult) SPS patients revealed no PAH.
Conclusions: These data indicate that TBX4 mutations are associated with childhood-onset PAH, but that the prevalence of PAH in adult TBX4 mutation carriers is low.
Keywords: Clinical genetics; Copy-number; Developmental; Molecular genetics; Pulmonary hypertension.
Figures
References
-
- Simonneau G, Robbins IM, Beghetti M, Channick RN, Delcroix M, Denton CP, Elliott CG, Gaine SP, Gladwin MT, Jing ZC, Krowka MJ, Langleben D, Nakanishi N, Souza R. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol 2009;54:S43–54 - PubMed
-
- Lane KB, Machado RD, Pauciulo MW, Thomson JR, Phillips JA, III, Loyd JE, Nichols WC, Trembath RC. Heterozygous germline mutations in BMPR2, encoding a TGF-beta receptor, cause familial primary pulmonary hypertension. Nat Genet 2000;26:81–4 - PubMed
-
- Trembath RC, Thomson JR, Machado RD, Morgan NV, Atkinson C, Winship I, Simonneau G, Galie N, Loyd JE, Humbert M, Nichols WC, Morrell NW, Berg J, Manes A, McGaughran J, Pauciulo M, Wheeler L. Clinical and molecular genetic features of pulmonary hypertension in patients with hereditary hemorrhagic telangiectasia. N Engl J Med 2001;345:325–34 - PubMed
-
- Trembath RC. Mutations in the TGF-beta type 1 receptor, ALK1, in combined primary pulmonary hypertension and hereditary haemorrhagic telangiectasia, implies pathway specificity. J Heart Lung Transplant 2001;20:175. - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous