

Cost-effectiveness of Quantiferon®-TB Gold-in-Tube versus tuberculin skin testing for contact screening and treatment of latent tuberculosis infection in Brazil
- PMID: 23593145
- PMCID: PMC3617186
- DOI: 10.1371/journal.pone.0059546
Cost-effectiveness of Quantiferon®-TB Gold-in-Tube versus tuberculin skin testing for contact screening and treatment of latent tuberculosis infection in Brazil
Abstract
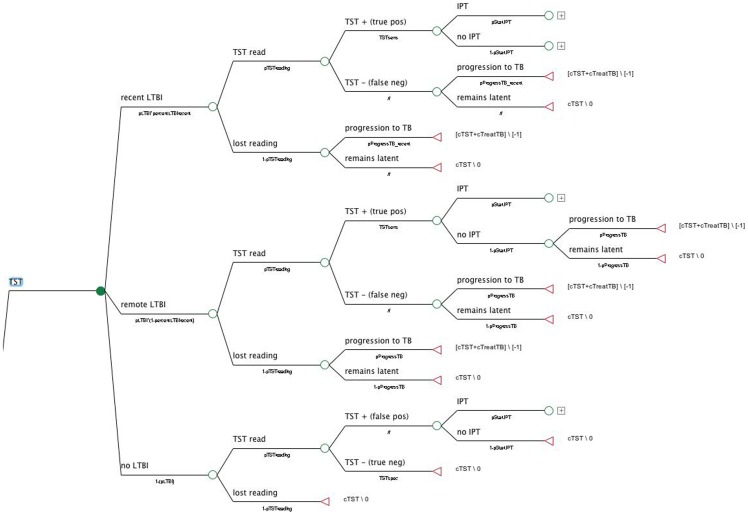
Background: Latent tuberculosis infection (LTBI) is a reservoir for new TB cases. Isoniazid preventive therapy (IPT) reduces the risk of active TB by as much as 90%, but LTBI screening has limitations. Unlike tuberculin skin testing (TST), interferon-gamma release assays are not affected by BCG vaccination, and have been reported to be cost-effective in low-burden countries. The goal of this study was to perform a cost-effectiveness analysis from the health system perspective, comparing three strategies for LTBI diagnosis in TB contacts: tuberculin skin testing (TST), QuantiFERON®-TB Gold-in-Tube (QFT-GIT) and TST confirmed by QFT-GIT if positive (TST/QFT-GIT) in Brazil, a middle-income, high-burden country with universal BCG coverage.
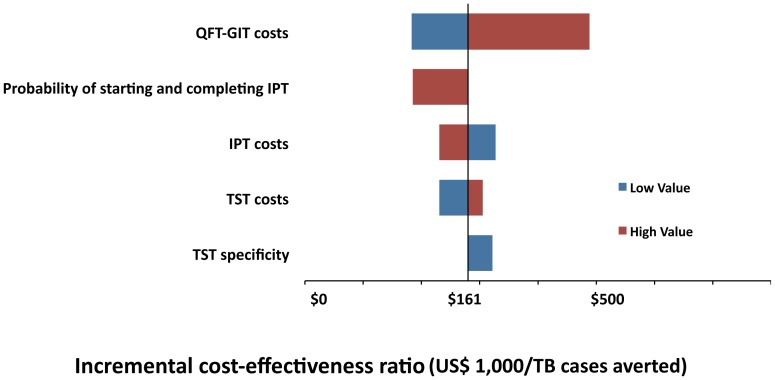
Methodology/principal findings: Costs for LTBI diagnosis and treatment of a hypothetical cohort of 1,000 adult immunocompetent close contacts were considered. The effectiveness measure employed was the number of averted TB cases in two years. Health system costs were US$ 105,096 for TST, US$ 121,054 for QFT-GIT and US$ 101,948 for TST/QFT-GIT; these strategies averted 6.56, 6.63 and 4.59 TB cases, respectively. The most cost-effective strategy was TST (US$ 16,021/averted case). The incremental cost-effectiveness ratio was US$ 227,977/averted TB case for QFT-GIT. TST/QFT-GIT was dominated.
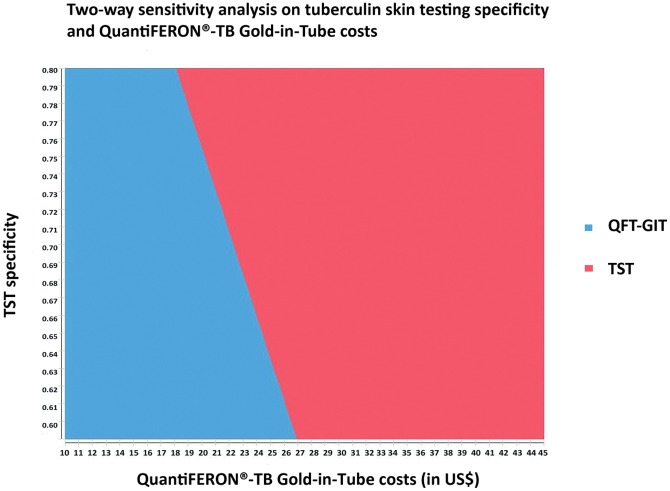
Conclusions: Unlike previous studies, TST was the most cost-effective strategy for averting new TB cases in the short term. QFT-GIT would be more cost-effective if its costs could be reduced to US$ 26.95, considering a TST specificity of 59% and US$ 18 considering a more realistic TST specificity of 80%. Nevertheless, with TST, 207.4 additional people per 1,000 will be prescribed IPT compared with QFT.
Conflict of interest statement
Figures
References
-
- Raviglione M, Marais B, Floyd K, Lonnroth K, Getahun H, et al. (2012) Scaling up interventions to achieve global tuberculosis control: progress and new developments. Lancet 379: 1902–1913. - PubMed
-
- Dye C, Watt CJ, Bleed DM, Hosseini SM, Raviglione MC (2005) Evolution of tuberculosis control and prospects for reducing tuberculosis incidence, prevalence, and deaths globally. JAMA 293: 2767–2775. - PubMed
-
- Menzies D, Gardiner G, Farhat M, Greenaway C, Pai M (2008) Thinking in three dimensions: a web-based algorithm to aid the interpretation of tuberculin skin test results. Int J Tuberc Lung Dis 12: 498–505. - PubMed
-
- International Union Against Tuberculosis Committee on Prophylaxis (1982) Efficacy of various durations of isoniazid preventive therapy for tuberculosis: five years of follow-up in the IUATL trial: International Union Against Tuberculosis Committee on Prophylaxis. Bull World Health Organ: 555–564. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
