

Retrospective analysis of prognostic factors in 205 patients with laryngeal squamous cell carcinoma who underwent surgical treatment
- PMID: 23593169
- PMCID: PMC3617169
- DOI: 10.1371/journal.pone.0060157
Retrospective analysis of prognostic factors in 205 patients with laryngeal squamous cell carcinoma who underwent surgical treatment
Abstract
Objectives: To investigate the most important factors affecting the prognosis of the patients with squamous cell carcinoma (SCC) of the larynx.
Methods: Based on the clinical and follow-up data, 205 patients with SCC of the larynx receiving total laryngectomy, partial laryngectomy, or CO2 laser surgery in GuangDong General Hospital were retrospectively analyzed. A survival analysis was performed by the Kaplan-Meier method and a multivariable analysis of prognostic factors was carried out using the Cox proportional hazard model.
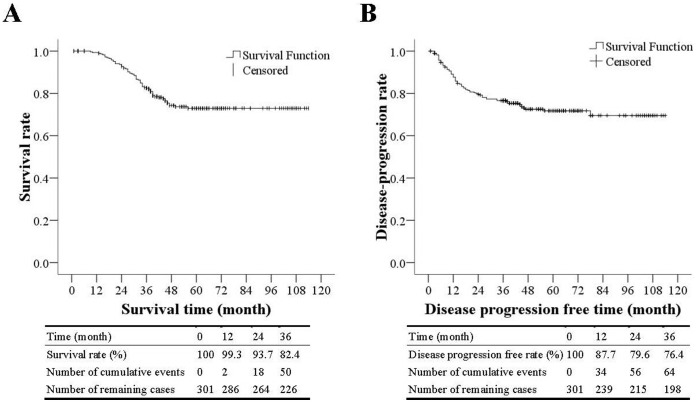
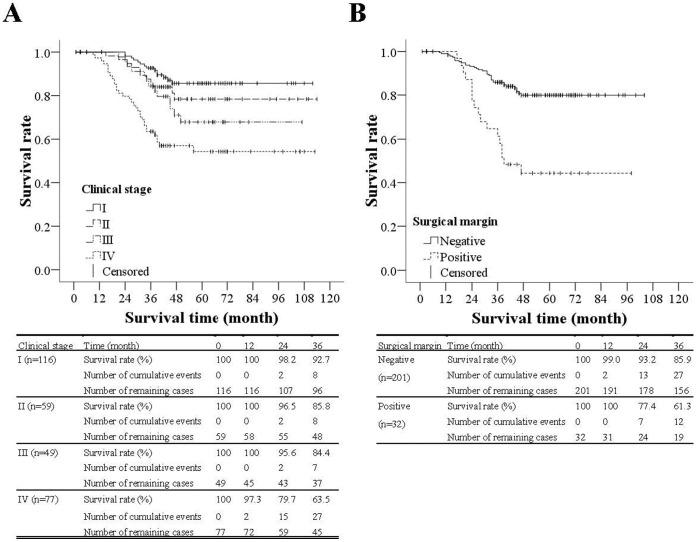
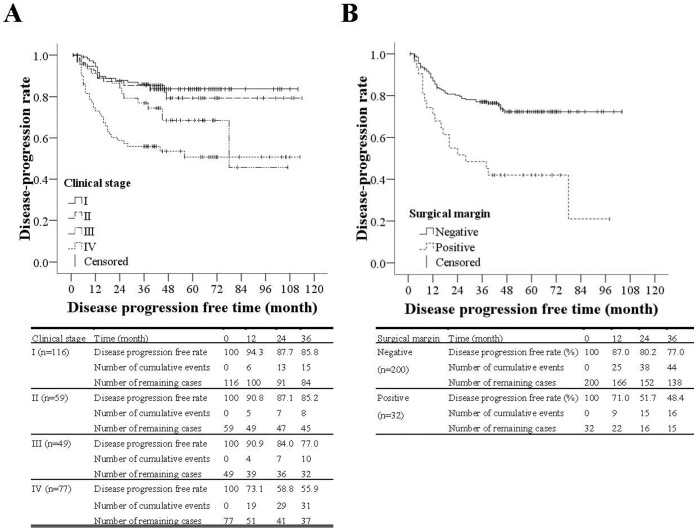
Results: Subtypes of carcinoma included 69.8% glottic and 30.2% supraglottic. Most patients were in N0 stage (77.6%), and 22.4% patients were in N1∼N3 stage. Over half of the patients were in T1∼T2 stage (55.1%), 20.0% in T3, and 24.9% in T4. Mean follow-up duration was 49.2 months. The survival rates 1, 2, and 3 years after the surgery were 99.0%, 91.7%, and 81.5%, respectively. The survival rate for those patients with clinical stage IV was significantly lower than for those with clinical stage I and II (p<0.001 and p = 0.013, respectively). The disease-free progression rates 1, 2, and 3 years after the surgery were 83.9%, 74.6%, and 71.2%, respectively. Futhermore, those patients with a Charlson score of 1 to 2 and ≥3 had higher risk of mortality than those with a Charlson score of 0 (hazard ratios of 1.8 and 2.41 p = 0.042 and p = 0.008). Multivariable analysis revealed that clinical stage, surgical margin, and comorbidity were significantly associated with both mortality and disease-free progression.
Conclusion: The surgical resection margin, clinical stage, and comorbidity were independent factors affecting the laryngeal cancer prognosis. The survival rates were lower for patients with advanced laryngeal cancer, positive surgical margins, or severe comorbidity, suggesting the importance of early diagnosis, early treatment, negative surgical margins, and conditions of comorbidity.
Conflict of interest statement
Figures
References
-
- Lin HW, Bhattacharyya N (2008) Staging and survival analysis for nonsquamous cell carcinomas of the larynx. Laryngoscope 118: 1003–1013. - PubMed
-
- Lu ST, Wei KR, Yu BH, Chen ZX, Liang ZH, et al. (2004) Analysis of laryngeal cancer incidence rate in Zhongshan City in 1970–1999. J Modern Oncology 12: 158–160.
-
- Hashibe M, Boffetta P, Zaridze D, Shangina O, Szeszenia-Dabrowska N, et al. (2007) Contribution of tobacco and alcohol to the high rates of squamous cell carcinoma of the supraglottis and glottis in Central Europe. Am J Epidemiol 165: 814–820. - PubMed
-
- Bianchini C, Pastore A, Pelucchi S, Torreggiani E, Lambertini E, et al. (2008) Sex hormone receptor levels in laryngeal carcinoma: a comparison between protein and RNA evaluations. Eur Arch Otorhinolaryngol 265: 1089–1094. - PubMed
-
- Shangina O, Brennan P, Szeszenia-Dabrowska N, Mates D, Fabianova E, et al. (2006) Occupational exposure and laryngeal and hypopharyngeal cancer risk in central and eastern Europe. Am J Epidemiol 164: 367–375. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
