

Asthma management in pregnancy
- PMID: 23593182
- PMCID: PMC3617219
- DOI: 10.1371/journal.pone.0060247
Asthma management in pregnancy
Abstract
Background: Asthma is common during pregnancy, however research is limited regarding the extent and timing of changes in asthma management associated with pregnancy.
Objective: To determine the prevalence of asthma during pregnancy and identify changes in treatment and asthma exacerbation rates associated with pregnancy, while controlling for seasonal influences.
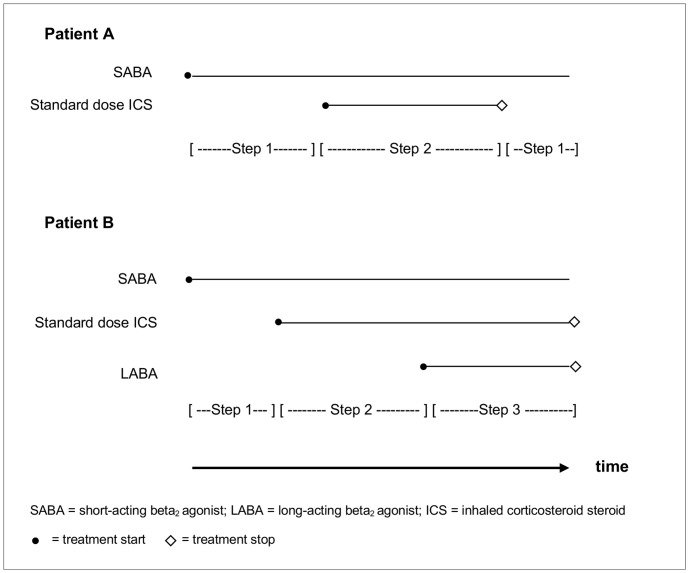
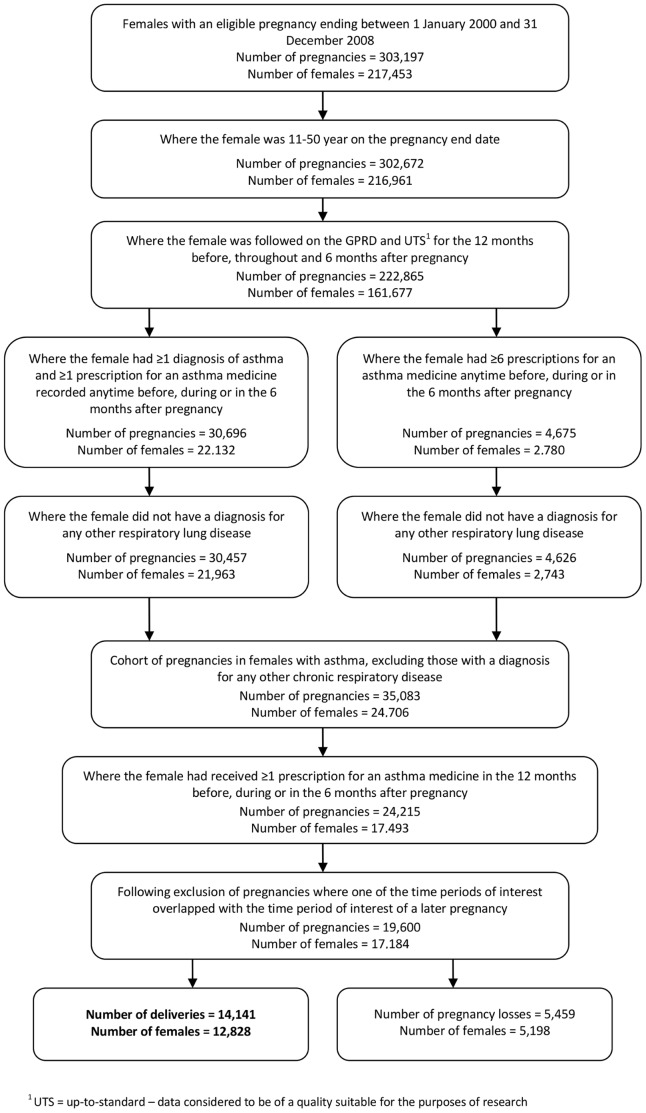
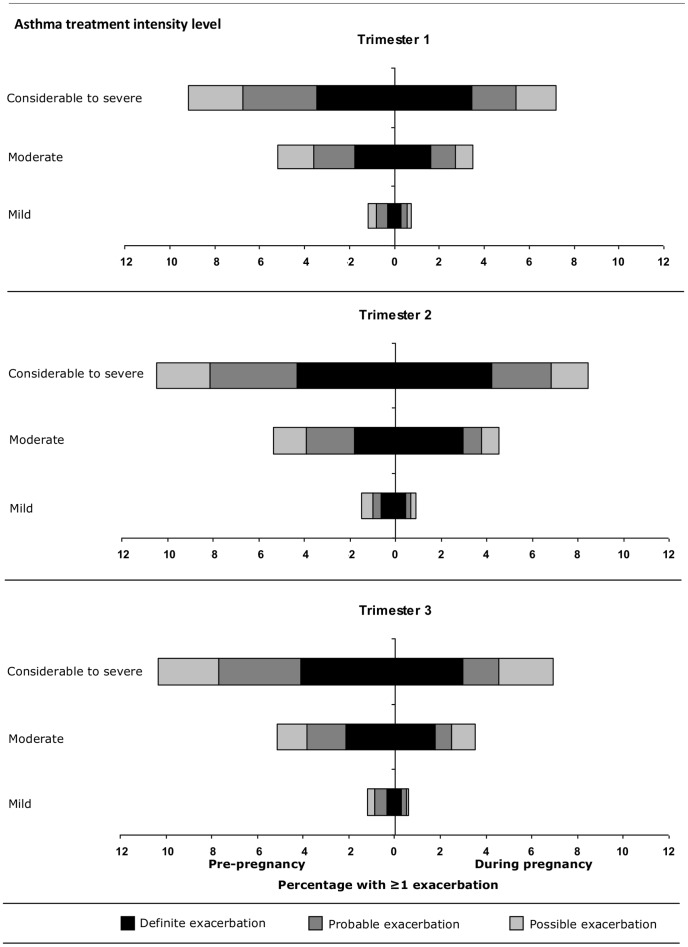
Methods: Pregnant women with asthma were identified from the UK General Practice Research Database between 2000 and 2008. For each woman asthma medication prescribed during the study period was identified; for each product combination the British Thoracic Society medication-defined asthma treatment step was identified. Asthma exacerbations were identified during pregnancy and in the corresponding 12 months prior. Analyses of changes in asthma treatment and exacerbation rates during pregnancy relative to the corresponding period 12 months prior, to control for seasonality, were stratified by trimester and asthma treatment intensity level.
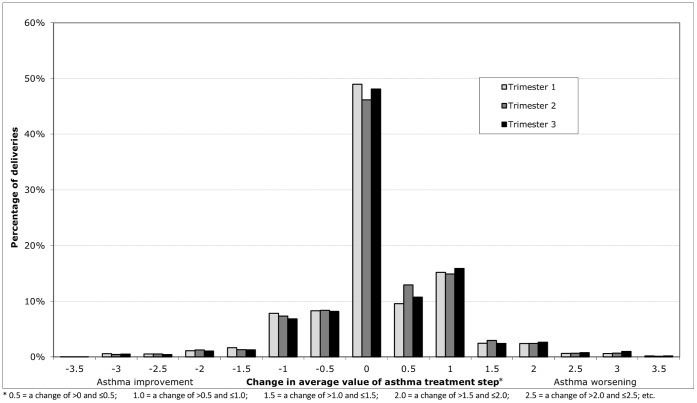
Results: The prevalence of treated asthma in pregnancies resulting in a delivery was 8.3%. From 14,141 pregnancies, in 12,828 women with asthma, 68.4% received prescriptions for a short-acting β2-agonist and 41.2% for inhaled corticosteroids; 76.5% were managed with asthma treatment Step 1 or 2. Poor persistence to inhaled corticosteroids, defined as a gap of up to 60 days between prescriptions, was common. In 45.0% of pregnancies, an increase in average treatment step was observed whereas in 25.6% the treatment step decreased. Treatment intensity remained the same in 29.5% of pregnancies. Exacerbations occurred in 4.8% of pregnancies compared to 5.9% in the same season the year before (p<0.001).
Conclusion: Exacerbation rates during pregnancy were slightly lower than in the year before. However, treatment patterns and exacerbation rates in this study suggest asthma control during pregnancy is variable, and women may require close monitoring especially in those with evidence of poor control before pregnancy.
Conflict of interest statement
Figures
References
-
- Kwon HL, Belanger K, Bracken MB (2003) Asthma Prevalence among Pregnant and Childbearing-aged Women in the United States: Estimates from National Health Surveys. Annals of Epidemiology 13: 317–324. - PubMed
-
- Kurinczuk JJ, Parsons DE, Dawes V, Burton PR (1999) The Relationship Between Asthma and Smoking During Pregnancy. Women & Health 29: 31–47. - PubMed
-
- Cleary BJ, Butt H, Strawbridge JD, Gallagher PJ, Fahey T, et al. (2010) Medication use in early pregnancy-prevalence and determinants of use in a prospective cohort of women. Pharmacoepidemiol Drug Saf 19: 408–417. - PubMed
-
- Dombrowski M (2006) Asthma and pregnancy. Obstet Gynecol 108: 667–681. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
