

A prospective study of the causes of febrile illness requiring hospitalization in children in Cambodia
- PMID: 23593267
- PMCID: PMC3621876
- DOI: 10.1371/journal.pone.0060634
A prospective study of the causes of febrile illness requiring hospitalization in children in Cambodia
Erratum in
-
Correction: A prospective study of the causes of febrile illness requiring hospitalization in children in Cambodia.PLoS One. 2015 Mar 26;10(3):e0119976. doi: 10.1371/journal.pone.0119976. eCollection 2015. PLoS One. 2015. PMID: 25811600 Free PMC article.
Abstract
Background: Febrile illnesses are pre-eminent contributors to morbidity and mortality among children in South-East Asia but the causes are poorly understood. We determined the causes of fever in children hospitalised in Siem Reap province, Cambodia.
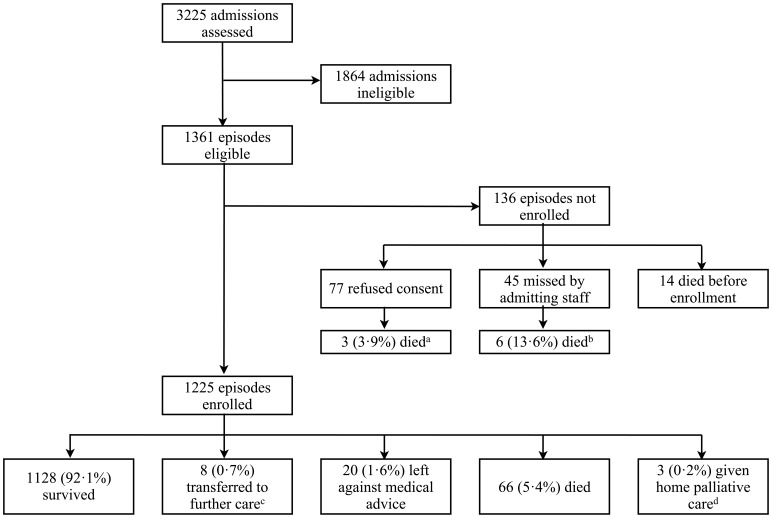
Methods and findings: A one-year prospective study of febrile children admitted to Angkor Hospital for Children, Siem Reap. Demographic, clinical, laboratory and outcome data were comprehensively analysed. Between October 12(th) 2009 and October 12(th) 2010 there were 1225 episodes of febrile illness in 1180 children. Median (IQR) age was 2.0 (0.8-6.4) years, with 850 (69%) episodes in children <5 years. Common microbiological diagnoses were dengue virus (16.2%), scrub typhus (7.8%), and Japanese encephalitis virus (5.8%). 76 (6.3%) episodes had culture-proven bloodstream infection, including Salmonella enterica serovar Typhi (22 isolates, 1.8%), Streptococcus pneumoniae (13, 1.1%), Escherichia coli (8, 0.7%), Haemophilus influenzae (7, 0.6%), Staphylococcus aureus (6, 0.5%) and Burkholderia pseudomallei (6, 0.5%). There were 69 deaths (5.6%), including those due to clinically diagnosed pneumonia (19), dengue virus (5), and melioidosis (4). 10 of 69 (14.5%) deaths were associated with culture-proven bloodstream infection in logistic regression analyses (odds ratio for mortality 3.4, 95% CI 1.6-6.9). Antimicrobial resistance was prevalent, particularly in S. enterica Typhi, (where 90% of isolates were resistant to ciprofloxacin, and 86% were multi-drug resistant). Comorbid undernutrition was present in 44% of episodes and a major risk factor for acute mortality (OR 2.1, 95% CI 1.1-4.2), as were HIV infection and cardiac disease.
Conclusion: We identified a microbiological cause of fever in almost 50% of episodes in this large study of community-acquired febrile illness in hospitalized children in Cambodia. The range of pathogens, antimicrobial susceptibility, and co-morbidities associated with mortality described will be of use in the development of rational guidelines for infectious disease treatment and control in Cambodia and South-East Asia.
Conflict of interest statement
Figures
References
-
- Liu L, Johnson HL, Cousens S, Perin J, Scott S, et al. (2012) Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet 379: 2151–61. - PubMed
-
- Bhutta ZA, Ali S, Cousens S, Ali TM, Azra Haider B, et al. (2008) Alma-Ata: Rebirth and revision 6 interventions to address maternal, newborn, and child survival: What difference can integrated primary health care strategies make? Lancet 372: 972–89. - PubMed
-
- Peacock SJ, Newton PN (2008) Public health impact of establishing the cause of bacterial infections in rural Asia. Trans R Soc Trop Med Hyg 102(1): 5–6. - PubMed
-
- Deen J, von Seidlein L, Andersen F, Elle N, White NJ, et al. (2012) Community-acquired bloodstream infections in developing countries in south and southeast Asia: a systematic review. Lancet Inf Dis 12: 480–87. - PubMed
-
- World Health Organization (2005) Handbook: Integrated management of childhood illness. Geneva, Switzerland: World Health Organization.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
