Management of aneurysms of the proximal (A1) segment of the anterior cerebral artery
- PMID: 23593600
- PMCID: PMC3625815
- DOI: 10.7461/jcen.2013.15.1.13
Management of aneurysms of the proximal (A1) segment of the anterior cerebral artery
Abstract
Objective: Aneurysms originating from the proximal segment (A1) of the anterior cerebral artery are rare; however, because of their small size, the risk of injury of perforating arteries, and the location of the aneurysm in the surgical field, they are challenging to treat. We report on 15 patients with A1 aneurysms and review surgical views according to the direction of aneurysms.
Methods: Fifteen patients were diagnosed with A1 aneurysms and underwent surgical clipping or endovascular coiling at our institution between January 2006 and March 2012. We conducted a retrospective review of clinical and radiological features of all patients with A1 aneurysms.
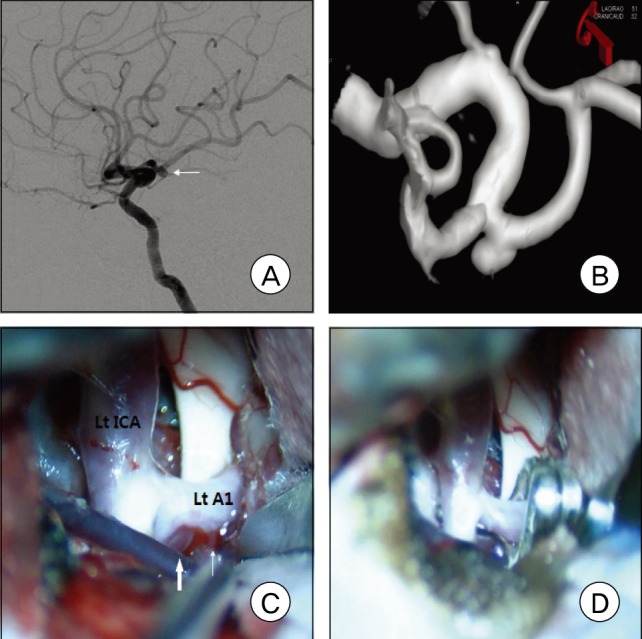
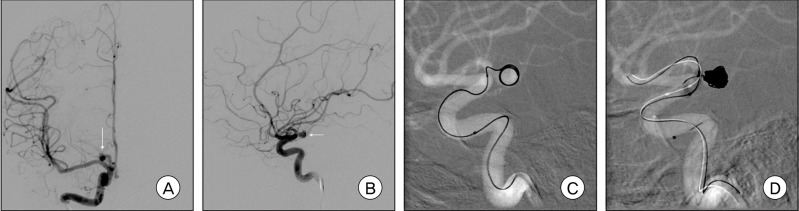
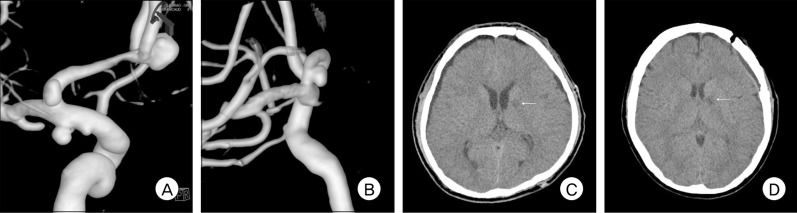
Results: Nine patients underwent surgical clipping, and six patients received endovascular coiling. Six patients (40%) had multiple aneurysms. A1 aneurysms ranged in size from 1.5 to 8.2 mm, with an average size of 3.26 mm. Most A1 aneurysms (73%) had a posterior direction. In the surgical view, A1 aneurysms projecting posteriorly were located behind the A1 trunk. The A1 aneurysm projecting posteroinferiorly was completely eclipsed by the parent artery. In A1 aneurysms with a posterosuperior or superior direction, finding and clipping the aneurysm neck was relatively easy. Thirteen patients (87%) had an excellent outcome, one had moderate disability, and one died.
Conclusion: A1 aneurysms have certain characteristics; small size, multiple aneurysms, and, usually, a posterior direction. A1 aneurysms with a posterosuperior or superior direction are relatively easy to assess, however, clipping of A1 aneurysms with a posterior or posteroinferior direction is more difficult. Endovascular coiling is an alternative therapeutic option when surgical clipping is expected to be difficult.
Keywords: Aneurysm; Angiography; Anterior cerebral artery; Proximal; Subarachnoid hemorrhage.
Figures


Similar articles
-
Radiographic and microsurgical characteristics of proximal (A1) segment aneurysms of the anterior cerebral artery.Neurol Sci. 2018 Oct;39(10):1735-1740. doi: 10.1007/s10072-018-3492-1. Epub 2018 Jul 10. Neurol Sci. 2018. PMID: 29987435
-
Microvascular Clipping of A1 Segment Aneurysms.Neurol India. 2019 Sep-Oct;67(5):1257-1263. doi: 10.4103/0028-3886.271266. Neurol India. 2019. PMID: 31744954
-
Characteristics and surgery of aneurysms of the proximal (A1) segment of the anterior cerebral artery.J Neurosurg Sci. 2005 Sep;49(3):85-95. J Neurosurg Sci. 2005. PMID: 16288191
-
Surgery of proximal anterior cerebral artery aneurysms.Acta Neurochir (Wien). 2002 Dec;144(12):1291-6; discussion 1296. doi: 10.1007/s00701-002-1014-6. Acta Neurochir (Wien). 2002. PMID: 12478340 Review.
-
Ruptured carotid-ophthalmic aneurysm treatment: a non-inferiority meta-analysis comparing endovascular coiling and surgical clipping.Br J Neurosurg. 2017 Jun;31(3):345-349. doi: 10.1080/02688697.2017.1297371. Epub 2017 Mar 2. Br J Neurosurg. 2017. PMID: 28637115 Review.
Cited by
-
Blister-like Cerebral Aneurysm after Endovascular Catheterization: A Case Report and Literature Review.Cureus. 2023 May 29;15(5):e39674. doi: 10.7759/cureus.39674. eCollection 2023 May. Cureus. 2023. PMID: 37398705 Free PMC article.
-
Contemporaneous Clipping of Unruptured Anterior Cerebral Artery Proximal A1 Segment Aneurysm and Resection of Dural-Based Brain Tumor.Cureus. 2020 May 18;12(5):e8183. doi: 10.7759/cureus.8183. Cureus. 2020. PMID: 32566424 Free PMC article.
-
Morphological and Hemodynamic Risk Factors for the Rupture of Proximal Anterior Cerebral Artery Aneurysms (A1 Segment).Front Aging Neurosci. 2022 Feb 18;14:835373. doi: 10.3389/fnagi.2022.835373. eCollection 2022. Front Aging Neurosci. 2022. PMID: 35250548 Free PMC article.
-
Radiographic and microsurgical characteristics of proximal (A1) segment aneurysms of the anterior cerebral artery.Neurol Sci. 2018 Oct;39(10):1735-1740. doi: 10.1007/s10072-018-3492-1. Epub 2018 Jul 10. Neurol Sci. 2018. PMID: 29987435
-
A Rare Case of Unruptured Small Aneurysm Arising from the Posterior Surface of Proximal A1 Segment, Projecting Posterior-Inferiorly and Entangled with Multiple Perforators from the A1 Segment.Asian J Neurosurg. 2024 Jul 4;19(3):536-539. doi: 10.1055/s-0043-1776990. eCollection 2024 Sep. Asian J Neurosurg. 2024. PMID: 39205894 Free PMC article.
References
-
- Chang HW, Youn SW, Jung C, Kang HS, Sohn CH, Kwon BJ, et al. Technical strategy in endovascular treatment of proximal anterior cerebral artery aneurysms. Acta Neurochir (Wien) 2011 Feb;153(2):279–285. - PubMed
-
- Czepko R, Libionka W, Lopatka P. Characteristics and surgery of aneurysms of the proximal (A1) segment of the anterior cerebral artery. J Neurosurg Sci. 2005 Sep;49(3):85–95. - PubMed
-
- Dashti R, Hernesniemi J, Lehto H, Niemelä M, Lehecka M, Rinne J, et al. Microneurosurgical management of proximal anterior cerebral artery aneurysms. Surg Neurol. 2007 Oct;68(4):366–377. - PubMed
-
- Dunker RO, Harris AB. Surgical anatomy of the proximal anterior cerebral artery. J Neurosurg. 1976 Mar;44(3):359–367. - PubMed
-
- Gupta R, Horowitz MB, Gilman S. Neuroform stent-assisted coil embolization of a ruptured A1 segment anterior cerebral artery aneurysm. J Neuroimaging. 2006 Apr;16(2):117–119. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources