

Clinical features and outcomes of gastric variceal bleeding: retrospective Korean multicenter data
- PMID: 23593608
- PMCID: PMC3622854
- DOI: 10.3350/cmh.2013.19.1.36
Clinical features and outcomes of gastric variceal bleeding: retrospective Korean multicenter data
Abstract
Background/aims: While gastric variceal bleeding (GVB) is not as prevalent as esophageal variceal bleeding, it is reportedly more serious, with high failure rates of the initial hemostasis (>30%), and has a worse prognosis than esophageal variceal bleeding. However, there is limited information regarding hemostasis and the prognosis for GVB. The aim of this study was to determine retrospectively the clinical outcomes of GVB in a multicenter study in Korea.
Methods: The data of 1,308 episodes of GVB (males:females=1062:246, age=55.0±11.0 years, mean±SD) were collected from 24 referral hospital centers in South Korea between March 2003 and December 2008. The rates of initial hemostasis failure, rebleeding, and mortality within 5 days and 6 weeks of the index bleed were evaluated.
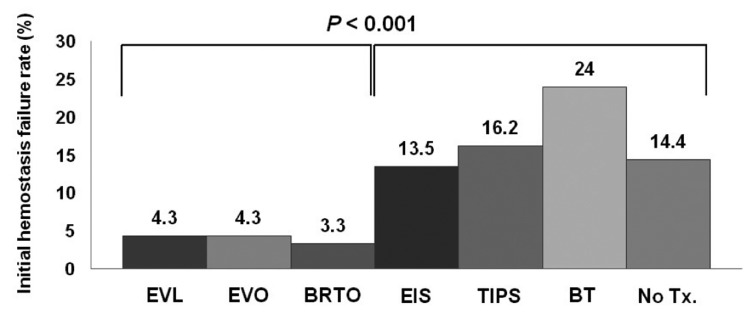
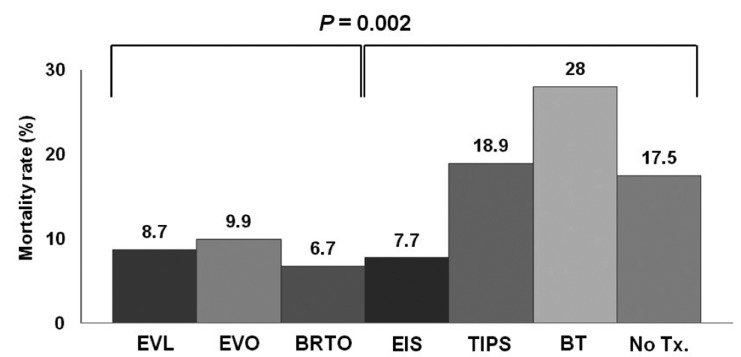
Results: The initial hemostasis failed in 6.1% of the patients, and this was associated with the Child-Pugh score [odds ratio (OR)=1.619; P<0.001] and the treatment modality: endoscopic variceal ligation, endoscopic variceal obturation, and balloon-occluded retrograde transvenous obliteration vs. endoscopic sclerotherapy, transjugular intrahepatic portosystemic shunt, and balloon tamponade (OR=0.221, P<0.001). Rebleeding developed in 11.5% of the patients, and was significantly associated with Child-Pugh score (OR=1.159, P<0.001) and treatment modality (OR=0.619, P=0.026). The GVB-associated mortality was 10.3%; mortality in these cases was associated with Child-Pugh score (OR=1.795, P<0.001) and the treatment modality for the initial hemostasis (OR=0.467, P=0.001).
Conclusions: The clinical outcome for GVB was better for the present cohort than in previous reports. Initial hemostasis failure, rebleeding, and mortality due to GVB were universally associated with the severity of liver cirrhosis.
Keywords: Cirrhosis; Gastric variceal bleeding; Mortality; Rebleeding.
Conflict of interest statement
The authors have no conflicts to disclose.
Figures
Similar articles
-
Comparison of treatment outcomes between balloon-occluded retrograde transvenous obliteration and transjugular intrahepatic portosystemic shunt for gastric variceal bleeding hemostasis.J Gastroenterol Hepatol. 2017 Aug;32(8):1487-1494. doi: 10.1111/jgh.13729. J Gastroenterol Hepatol. 2017. PMID: 28085232
-
Can proton pump inhibitors reduce rebleeding following Histoacryl sclerotherapy for gastric variceal hemorrhage?Korean J Intern Med. 2015 Sep;30(5):593-601. doi: 10.3904/kjim.2015.30.5.593. Epub 2015 Aug 27. Korean J Intern Med. 2015. PMID: 26354053 Free PMC article.
-
Clinical outcomes of balloon-occluded retrograde transvenous obliteration for the treatment of gastric variceal hemorrhage in Korean patients with liver cirrhosis: a retrospective multicenter study.Clin Mol Hepatol. 2012 Dec;18(4):368-74. doi: 10.3350/cmh.2012.18.4.368. Epub 2012 Dec 21. Clin Mol Hepatol. 2012. PMID: 23323252 Free PMC article.
-
Gastroesophageal variceal bleeding - An overview of current treatment options.Acta Gastroenterol Belg. 2018 Apr-Jun;81(2):305-317. Acta Gastroenterol Belg. 2018. PMID: 30024703 Review.
-
Endoscopic variceal ligation compared with endoscopic injection sclerotherapy for treatment of esophageal variceal hemorrhage: a meta-analysis.World J Gastroenterol. 2015 Feb 28;21(8):2534-41. doi: 10.3748/wjg.v21.i8.2534. World J Gastroenterol. 2015. PMID: 25741164 Free PMC article. Review.
Cited by
-
The secondary prophylactic efficacy of beta-blocker after endoscopic gastric variceal obturation for first acute episode of gastric variceal bleeding.Clin Mol Hepatol. 2013 Sep;19(3):280-7. doi: 10.3350/cmh.2013.19.3.280. Epub 2013 Sep 30. Clin Mol Hepatol. 2013. PMID: 24133666 Free PMC article.
-
Plug-Assisted Retrograde Transvenous Obliteration for the Treatment of Gastric Varices: The Role of Intra-Procedural Cone-Beam Computed Tomography.Korean J Radiol. 2018 Mar-Apr;19(2):223-229. doi: 10.3348/kjr.2018.19.2.223. Epub 2018 Feb 22. Korean J Radiol. 2018. PMID: 29520179 Free PMC article.
-
Usefulness of intra-procedural cone-beam computed tomography in modified balloon-occluded retrograde transvenous obliteration of gastric varices.World J Radiol. 2016 Apr 28;8(4):390-6. doi: 10.4329/wjr.v8.i4.390. World J Radiol. 2016. PMID: 27158425 Free PMC article.
-
KASL clinical practice guidelines for liver cirrhosis: Varices, hepatic encephalopathy, and related complications.Clin Mol Hepatol. 2020 Apr;26(2):83-127. doi: 10.3350/cmh.2019.0010n. Epub 2020 Jan 10. Clin Mol Hepatol. 2020. PMID: 31918536 Free PMC article. No abstract available.
-
Effects of candesartan and propranolol combination therapy versus propranolol monotherapy in reducing portal hypertension.Clin Mol Hepatol. 2014 Dec;20(4):376-83. doi: 10.3350/cmh.2014.20.4.376. Epub 2014 Dec 24. Clin Mol Hepatol. 2014. PMID: 25548744 Free PMC article. Clinical Trial.
References
-
- Sarin SK, Lahoti D, Saxena SP, Murthy NS, Makwana UK. Prevalence, classification and natural history of gastric varices: a long-term follow-up study in 568 portal hypertension patients. Hepatology. 1992;16:1343–1349. - PubMed
-
- Thakeb F, Salem SA, Abdallah M, el Batanouny M. Endoscopic diagnosis of gastric varices. Endoscopy. 1994;26:287–291. - PubMed
-
- Trudeau W, Prindiville T. Endoscopic injection sclerosis in bleeding gastric varices. Gastrointest Endosc. 1986;32:264–268. - PubMed
-
- Sarin SK. Long-term follow-up of gastric variceal sclerotherapy: an eleven-year experience. Gastrointest Endosc. 1997;46:8–14. - PubMed
-
- Ryan BM, Stockbrugger RW, Ryan JM. A pathophysiologic, gastroenterologic, and radiologic approach to the management of gastric varices. Gastroenterology. 2004;126:1175–1189. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
