

Contribution of moxifloxacin or levofloxacin in second-line regimens with or without continuation of pyrazinamide in murine tuberculosis
- PMID: 23593945
- PMCID: PMC3735243
- DOI: 10.1164/rccm.201212-2328OC
Contribution of moxifloxacin or levofloxacin in second-line regimens with or without continuation of pyrazinamide in murine tuberculosis
Abstract
Rationale: High-dose levofloxacin (L) (1,000 mg) was as active as moxifloxacin (M) (400 mg) in an early bactericidal activity trial, suggesting these fluoroquinolones could be used interchangeably. Whether pyrazinamide (Z) contributes sterilizing activity beyond the first 2 months in fluoroquinolone-containing second-line regimens remains unknown.
Objectives: We compared the efficacy of M and high-dose L alone or in combination with ethionamide (Et), amikacin (A), and Z given for 2 or 7 months.
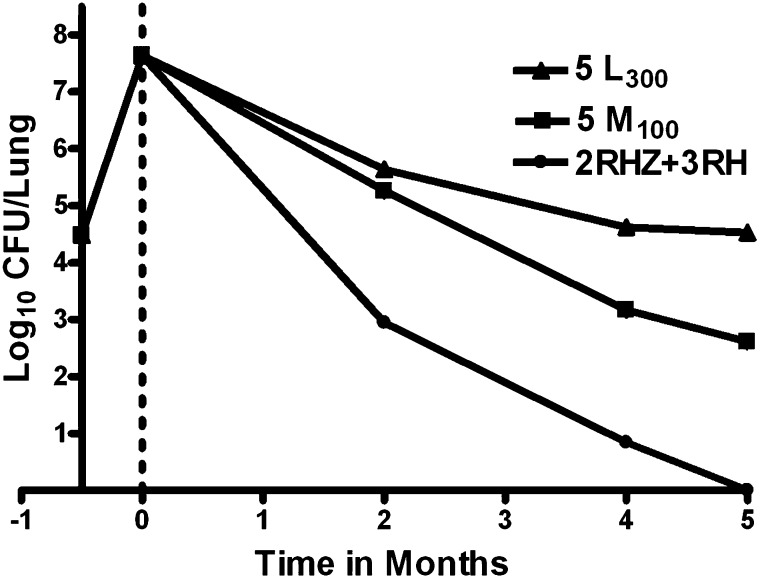
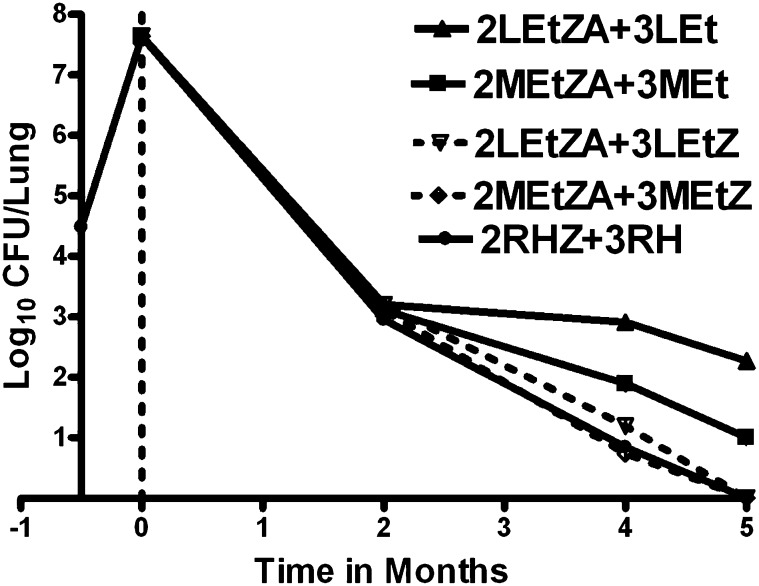
Methods: A pharmacokinetic study was performed to determine the L dose equivalent to 1,000 mg in humans. Treatment started 2 weeks after aerosol infection with Mycobacterium tuberculosis H37Rv. Mice received M or L alone or in combination with 2 months of EtZA followed by 5 months of Et or EtZ.
Measurements and main results: After 2 months of treatment, lung colony-forming unit (CFU) counts were similar in mice receiving either fluoroquinolone alone, but, after 4 and 5 months, CFU counts were 2 log10 lower in mice receiving M. Mice receiving 2MEtZA/3MEt and 2LEtZA/3LEt had 1.0 and 2.7 log10 lung CFUs, respectively. When Z was given throughout, both regimens rendered mice culture negative by 5 months, and most mice did not relapse after 7 months of treatment, with fewer relapses observed in the M group after 6 and 7 months of treatment.
Conclusions: In murine tuberculosis, M had superior efficacy compared with L despite lower serum drug exposures and may remain the fluoroquinolone of choice for second-line regimens. Z contributed substantial sterilizing activity beyond 2 months in fluoroquinolone-containing second-line regimens, largely compensating for L's weaker activity.
Figures
Comment in
-
Rationalizing use of fluoroquinolones and pyrazinamide in the battle against multidrug-resistant tuberculosis.Am J Respir Crit Care Med. 2013 Jul 1;188(1):10-1. doi: 10.1164/rccm.201304-0697ED. Am J Respir Crit Care Med. 2013. PMID: 23815718 No abstract available.
References
-
- Yew WW, Chan CK, Chau CH, Tam CM, Leung CC, Wong PC, Lee J. Outcomes of patients with multidrug-resistant pulmonary tuberculosis treated with ofloxacin/levofloxacin-containing regimens. Chest. 2000;117:744–751. - PubMed
-
- Chan ED, Laurel V, Strand MJ, Chan JF, Huynh ML, Goble M, Iseman MD. Treatment and outcome analysis of 205 patients with multidrug-resistant tuberculosis. Am J Respir Crit Care Med. 2004;169:1103–1109. - PubMed
-
- Tahaoglu K, Torun T, Sevim T, Atac G, Kir A, Karasulu L, Ozmen I, Kapakli N. The treatment of multidrug-resistant tuberculosis in Turkey. N Engl J Med. 2001;345:170–174. - PubMed
-
- Yew WW, Chan CK, Leung CC, Chau CH, Tam CM, Wong PC, Lee J. Comparative roles of levofloxacin and ofloxacin in the treatment of multidrug-resistant tuberculosis: preliminary results of a retrospective study from Hong Kong. Chest. 2003;124:1476–1481. - PubMed
-
- Rieder HL. Fourth-generation fluoroquinolones in tuberculosis. Lancet. 2009;373:1148–1149. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
