

Is there an association between elevated or low serum levels of phosphorus, parathyroid hormone, and calcium and mortality in patients with end stage renal disease? A meta-analysis
- PMID: 23594621
- PMCID: PMC3658973
- DOI: 10.1186/1471-2369-14-88
Is there an association between elevated or low serum levels of phosphorus, parathyroid hormone, and calcium and mortality in patients with end stage renal disease? A meta-analysis
Abstract
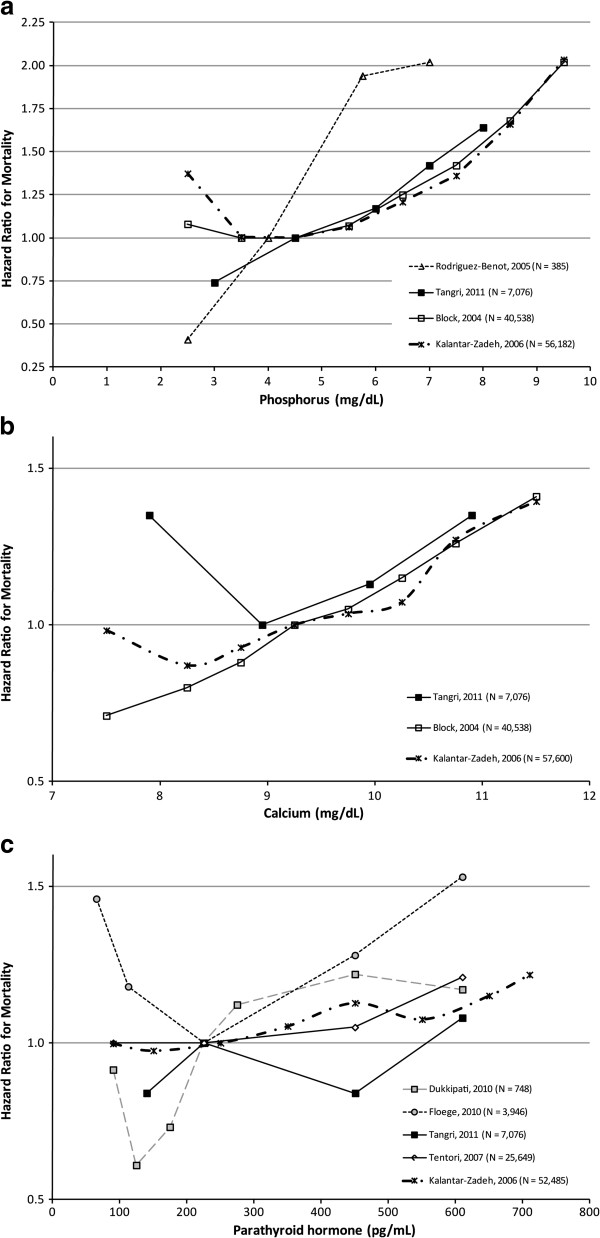
Background: Biochemical markers of altered mineral metabolism have been associated with increased mortality in end stage renal disease patients. Several studies have demonstrated non-linear (U-shaped or J-shaped) associations between these minerals and mortality, though many researchers have assumed linear relationships in their statistical modeling. This analysis synthesizes the non-linear relationships across studies.
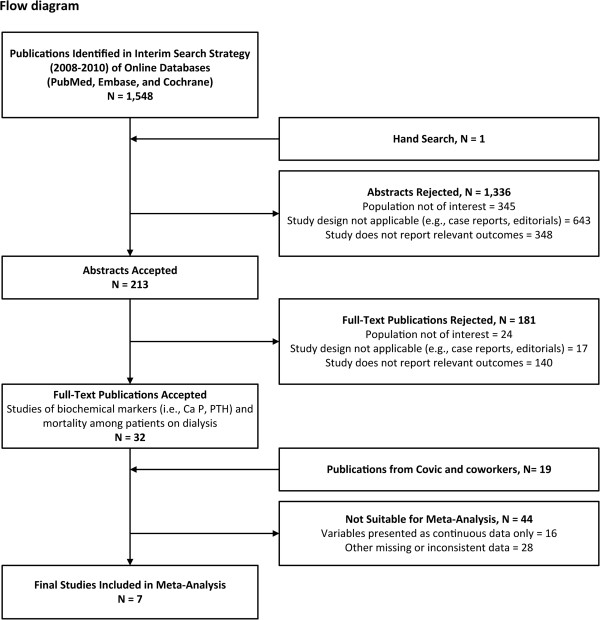
Methods: We updated a prior systematic review through 2010. Studies included adults receiving dialysis and reported categorical data for calcium, phosphorus, and/or parathyroid hormone (PTH) together with all-cause mortality. We performed 2 separate meta-analyses to compare higher-than-referent levels vs referent and lower-than-referent levels vs referent levels.
Results: A literature review showed that when a linear relationship between the minerals and mortality was assumed, the estimated associations were more likely to be smaller or non-significant compared to non-linear models. In the meta-analyses, higher-than-referent levels of phosphorus (4 studies, RR = 1.20, 95% CI = 1.15-1.25), calcium (3 studies, RR = 1.10, 95% CI = 1.05-1.14), and PTH (5 studies, RR = 1.11, 95% CI = 1.07-1.16) were significantly associated with increased mortality. Although no significant associations between relatively low phosphorus or PTH and mortality were observed, a protective effect was observed for lower-than-referent calcium (RR = 0.86, 95% CI = 0.83-0.89).
Conclusions: Higher-than-referent levels of PTH, calcium, and phosphorus in dialysis patients were associated with increased mortality risk in a selection of observational studies suitable for meta-analysis of non-linear relationships. Findings were less consistent for lower-than-referent values. Future analyses should incorporate the non-linear relationships between the minerals and mortality to obtain accurate effect estimates.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
