

Effect of a systems intervention on the quality and safety of patient handoffs in an internal medicine residency program
- PMID: 23595931
- PMCID: PMC3710376
- DOI: 10.1007/s11606-013-2391-7
Effect of a systems intervention on the quality and safety of patient handoffs in an internal medicine residency program
Abstract
Background: Poor quality handoffs have been identified as a major patient safety issue. In residency programs, problematic handoffs may be an unintended consequence of duty-hour restrictions, and key data are frequently omitted from written handoffs because of the lack of standardization of content.
Objective: Determine whether an intervention that facilitates face-to-face communication supported by an electronic template improves the quality and safety of handoffs.
Design: Before-after trial.
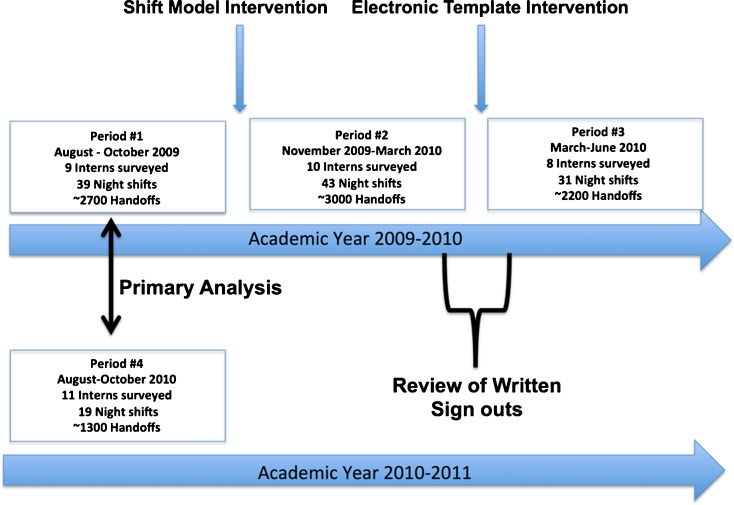
Participants: Thirty-nine interns providing nighttime coverage over 132 intern shifts, representing ∼9,200 handoffs.
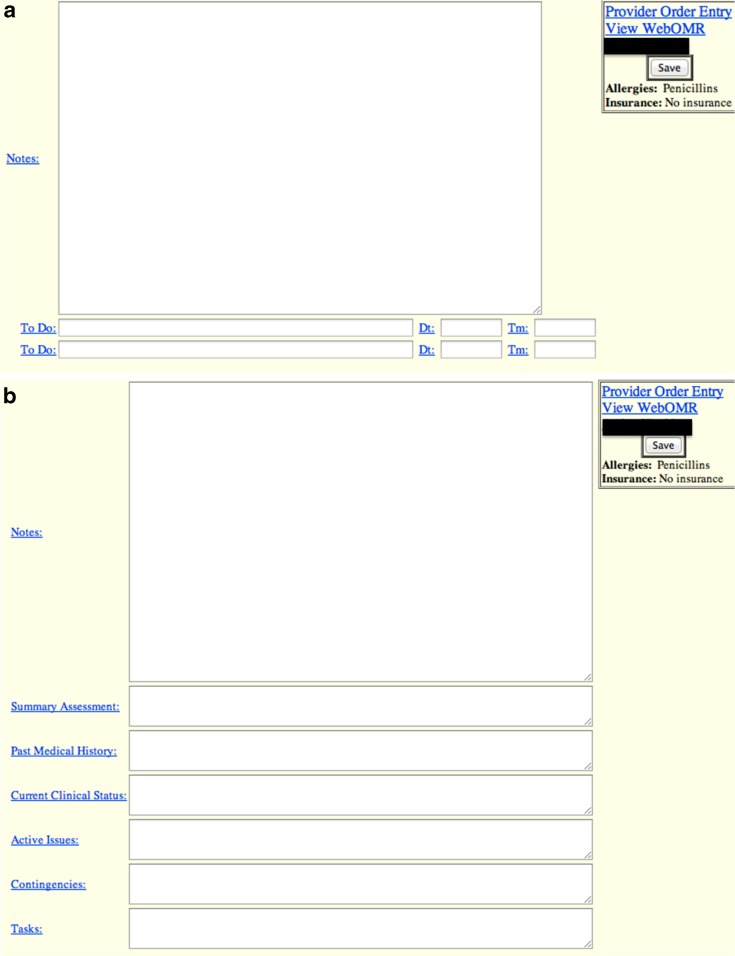
Interventions: Two interventions were implemented serially-an alteration of the shift model to facilitate face-to-face verbal communication between the primary and nighttime covering physicians and an electronic template for the day-to-night handoff.
Measurements: Overall satisfaction and handoff quality were measured using a survey tool administered at the end of each intern shift. Written handoff quality, specifically the documentation of key components, was also assessed before and after the template intervention by study investigators. Interns used the survey tool to report patient safety events related to poor quality handoffs, which were validated by study investigators.
Results: In adjusted analyses comparing intern cohorts with similar levels of training, overall satisfaction with the new handoff processes improved significantly (p < 0.001) post intervention. Verbal handoff quality (4/10 measures) and written handoff quality (5/6 measures) also improved significantly. Study investigators also found significant improvement in documentation of key components in the written handoff. Interns reported significantly fewer reported data omissions (p = 0.001) and a non-significant reduction in near misses (p = 0.056), but no significant difference in adverse events (p = 0.41) post intervention.
Conclusions: Redesign of shift models common in residency programs to minimize the number of handoffs and facilitate face-to-face communication, along with implementation of electronic handoff templates, improves the quality of handoffs in a learning environment.
Figures
Similar articles
-
Improving Handoffs: Implementing a Training Program for Incoming Internal Medicine Residents.J Grad Med Educ. 2018 Dec;10(6):698-701. doi: 10.4300/JGME-D-18-00244.1. J Grad Med Educ. 2018. PMID: 30619532 Free PMC article.
-
Rates of medical errors and preventable adverse events among hospitalized children following implementation of a resident handoff bundle.JAMA. 2013 Dec 4;310(21):2262-70. doi: 10.1001/jama.2013.281961. JAMA. 2013. PMID: 24302089
-
Content counts, but context makes the difference in developing expertise: a qualitative study of how residents learn end of shift handoffs.BMC Med Educ. 2018 Nov 3;18(1):249. doi: 10.1186/s12909-018-1350-8. BMC Med Educ. 2018. PMID: 30390668 Free PMC article.
-
Year-End Resident Clinic Handoffs: Narrative Review and Recommendations for Improvement.Jt Comm J Qual Patient Saf. 2017 Feb;43(2):71-79. doi: 10.1016/j.jcjq.2016.11.006. Epub 2016 Nov 15. Jt Comm J Qual Patient Saf. 2017. PMID: 28334565 Review.
-
Interunit handoffs from emergency department to inpatient care: A cross-sectional survey of physicians at a university medical center.J Hosp Med. 2015 Nov;10(11):711-7. doi: 10.1002/jhm.2431. Epub 2015 Jul 22. J Hosp Med. 2015. PMID: 26199192 Review.
Cited by
-
Artificial intelligence systems for complex decision-making in acute care medicine: a review.Patient Saf Surg. 2019 Feb 1;13:6. doi: 10.1186/s13037-019-0188-2. eCollection 2019. Patient Saf Surg. 2019. PMID: 30733829 Free PMC article. Review.
-
Technological Solutions to Improve Inpatient Handover in the Era of Artificial Intelligence: Scoping Review.J Med Internet Res. 2025 Jul 31;27:e70358. doi: 10.2196/70358. J Med Internet Res. 2025. PMID: 40743446 Free PMC article.
-
Improving residents' handovers through just-in-time training for structured communication.BMJ Qual Improv Rep. 2016 Feb 8;5(1):u209900.w4090. doi: 10.1136/bmjquality.u209900.w4090. eCollection 2016. BMJ Qual Improv Rep. 2016. PMID: 26893890 Free PMC article.
-
Evaluating Outcomes of Electronic Tools Supporting Physician Shift-to-Shift Handoffs: A Systematic Review.J Grad Med Educ. 2015 Jun;7(2):174-80. doi: 10.4300/JGME-D-14-00205.1. J Grad Med Educ. 2015. PMID: 26221430 Free PMC article.
-
Patient safety after implementation of a coproduced family centered communication programme: multicenter before and after intervention study.BMJ. 2018 Dec 5;363:k4764. doi: 10.1136/bmj.k4764. BMJ. 2018. PMID: 30518517 Free PMC article. Clinical Trial.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
