

Immune responses to AAV vectors: overcoming barriers to successful gene therapy
- PMID: 23596044
- PMCID: PMC3701904
- DOI: 10.1182/blood-2013-01-306647
Immune responses to AAV vectors: overcoming barriers to successful gene therapy
Abstract
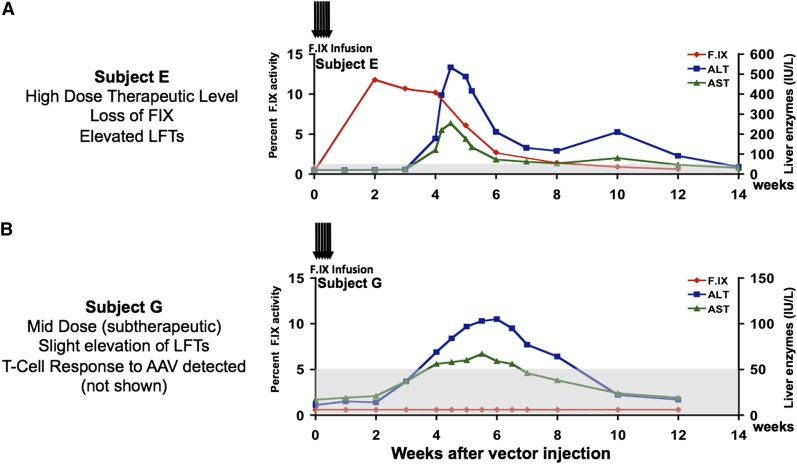
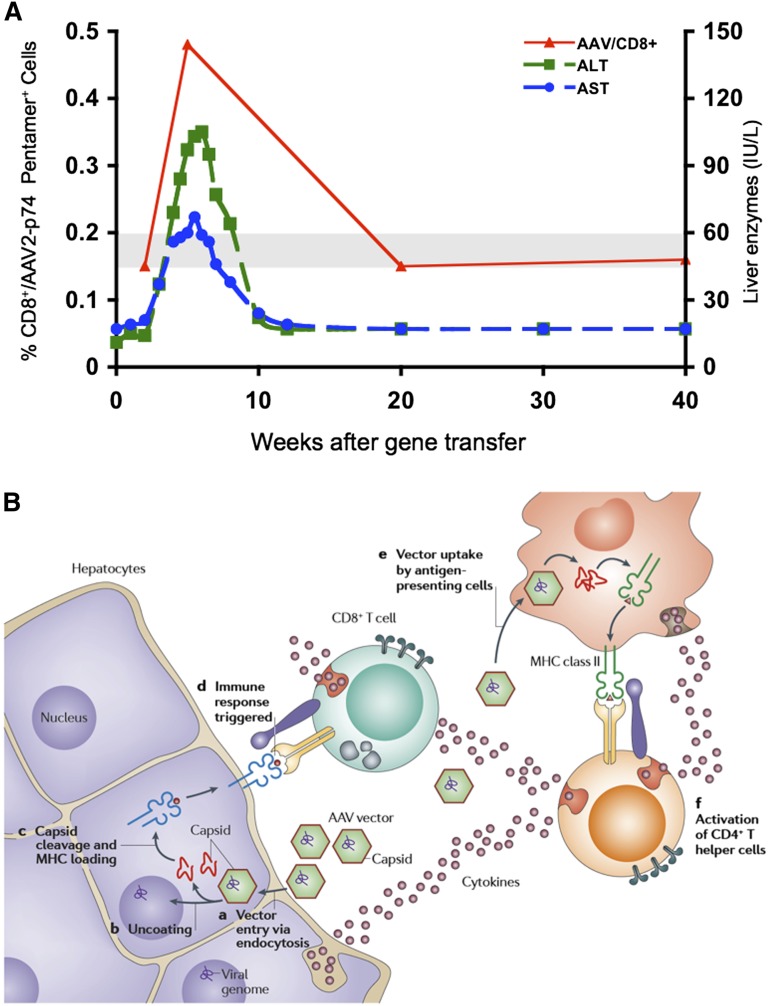
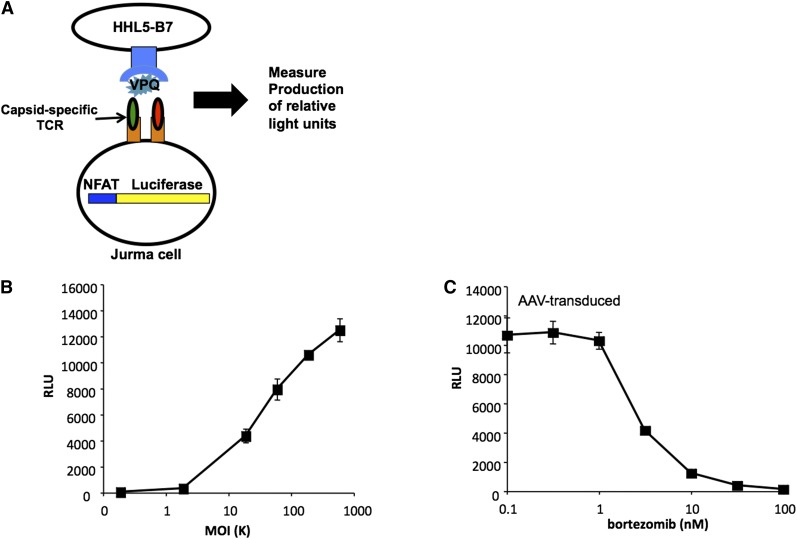
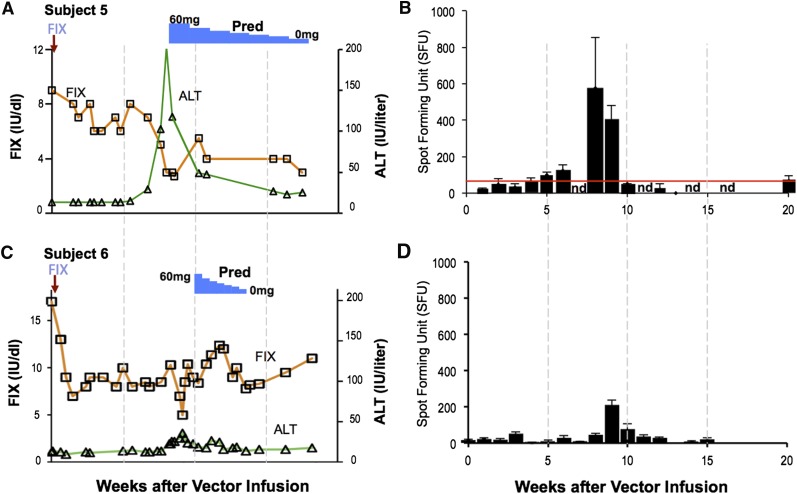
Gene therapy products for the treatment of genetic diseases are currently in clinical trials, and one of these, an adeno-associated viral (AAV) product, has recently been licensed. AAV vectors have achieved positive results in a number of clinical and preclinical settings, including hematologic disorders such as the hemophilias, Gaucher disease, hemochromatosis, and the porphyrias. Because AAV vectors are administered directly to the patient, the likelihood of a host immune response is high, as shown by human studies. Preexisting and/or recall responses to the wild-type virus from which the vector is engineered, or to the transgene product itself, can interfere with therapeutic efficacy if not identified and managed optimally. Small-scale clinical studies have enabled investigators to dissect the immune responses to the AAV vector capsid and to the transgene product, and to develop strategies to manage these responses to achieve long-term expression of the therapeutic gene. However, a comprehensive understanding of the determinants of immunogenicity of AAV vectors, and of potential associated toxicities, is still lacking. Careful immunosurveillance conducted as part of ongoing clinical studies will provide the basis for understanding the intricacies of the immune response in AAV-mediated gene transfer, facilitating safe and effective therapies for genetic diseases.
Figures

References
-
- Aiuti A, Cattaneo F, Galimberti S, et al. Gene therapy for immunodeficiency due to adenosine deaminase deficiency. N Engl J Med. 2009;360(5):447–458. - PubMed
-
- Cartier N, Hacein-Bey-Abina S, Bartholomae CC, et al. Hematopoietic stem cell gene therapy with a lentiviral vector in X-linked adrenoleukodystrophy. Science. 2009;326(5954):818–823. - PubMed
-
- Bainbridge JW, Smith AJ, Barker SS, et al. Effect of gene therapy on visual function in Leber’s congenital amaurosis. N Engl J Med. 2008;358(21):2231–2239. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
