

Decreasing severe pain and serious adverse events while moving intensive care unit patients: a prospective interventional study (the NURSE-DO project)
- PMID: 23597243
- PMCID: PMC3672726
- DOI: 10.1186/cc12683
Decreasing severe pain and serious adverse events while moving intensive care unit patients: a prospective interventional study (the NURSE-DO project)
Abstract
Introduction: A quality-improvement project was conducted to reduce severe pain and stress-related events while moving ICU-patients.
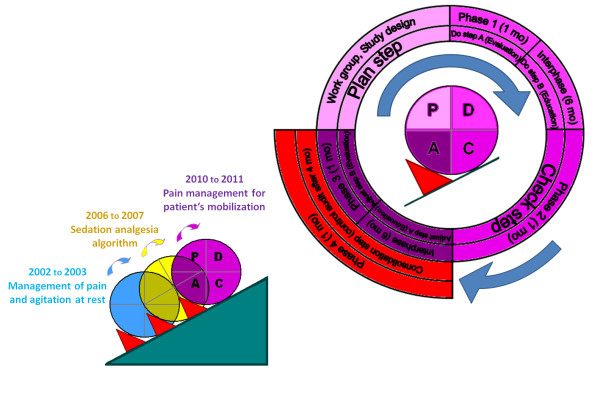
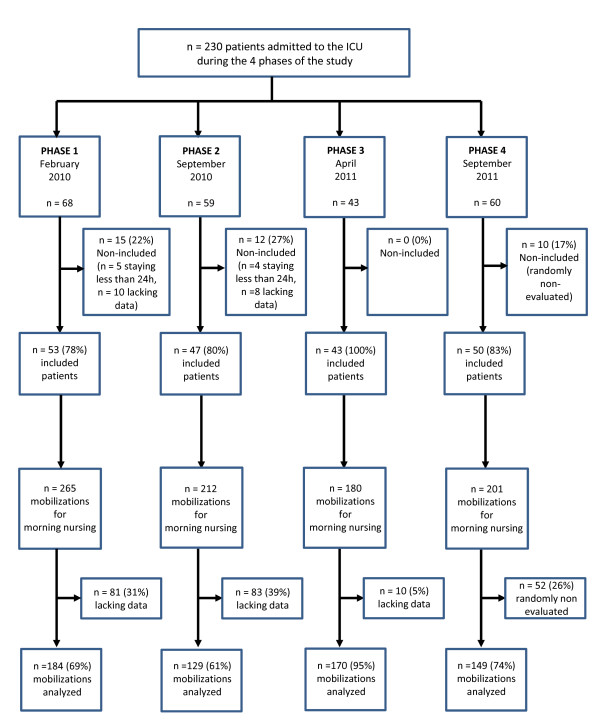
Methods: The Plan-Do-Check-Adjust cycle was studied during four one-month phases, separated by five-month interphases. All consecutive patients staying more than 24 hours were evaluated every morning while being moved for nursing care (bathing, massage, sheet-change, repositioning). Phase 1 was considered as the baseline. Implemented and adjusted quality-interventions were assessed at phases 2 and 3, respectively. An independent post-intervention control-audit was performed at Phase 4. Primary-endpoints were the incidence of severe pain defined by a behavioral pain scale > 5 or a 0 to 10 visual numeric rating scale > 6, and the incidence of serious adverse events (SAE): cardiac arrest, arrhythmias, tachycardia, bradycardia, hypertension, hypotension, desaturation, bradypnea or ventilatory distress. Pain, SAE, patients' characteristics and analgesia were compared among the phases by a multivariate mixed-effects model for repeated-measurements, adjusted on severity index, age, admission type (medical/surgical), intubation and sedation status.
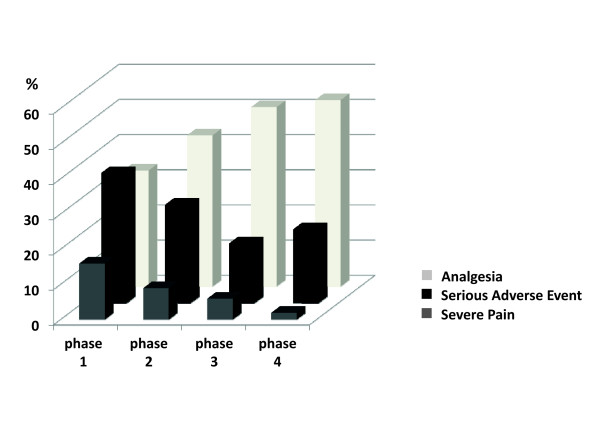
Results: During the four studied phases, 630 care procedures were analyzed in 53, 47, 43 and 50 patients, respectively. Incidence of severe pain decreased significantly from 16% (baseline) to 6% in Phase 3 (odds ratio (OR) = 0.33 (0.11; 0.98), P = 0.04) and 2% in Phase 4 (OR = 0.30 (0.12; 0.95), P = 0.02). Incidence of SAE decreased significantly from 37% (baseline) to 17% in Phase 3 and 21% in Phase 4. In multivariate analysis, SAE were independently associated with Phase 3 (OR = 0.40 (0.23; 0.72), P < 0.01), Phase 4 (OR = 0.53 (0.30; 0.92), P = 0.03), intubation status (OR = 1.91 (1.28; 2.85), P < 0.01) and severe pain (OR = 2.74 (1.54; 4.89), P < 0.001).
Conclusions: Severe pain and serious adverse events are common and strongly associated while moving ICU patients for nursing procedures. Quality improvement of pain management is associated with a decrease of serious adverse events. Careful documentation of pain management during mobilization for nursing procedures could be implemented as a health quality indicator in the ICU.
Figures
Comment in
-
Optimizing safe, comfortable ICU care through multi-professional quality improvement: just DO it.Crit Care. 2013 Apr 30;17(2):138. doi: 10.1186/cc12601. Crit Care. 2013. PMID: 23659656 Free PMC article.
References
-
- Chanques G, Sebbane M, Barbotte E, Viel E, Eledjam JJ, Jaber S. A prospective study of pain at rest: incidence and characteristics of an unrecognized symptom in surgical and trauma versus medical intensive care unit patients. Anesthesiology. 2007;107:858–860. doi: 10.1097/01.anes.0000287211.98642.51. - DOI - PubMed
-
- Payen JF, Chanques G, Mantz J, Hercule C, Auriant I, Leguillou JL, Binhas M, Genty C, Rolland C, Bosson JL. Current practices in sedation and analgesia for mechanically ventilated critically ill patients: a prospective multicenter patient-based study. Anesthesiology. 2007;106:687–695. doi: 10.1097/01.anes.0000264747.09017.da. - DOI - PubMed
-
- Lewis KS, Whipple JK, Michael KA, Quebbeman EJ. Effect of analgesic treatment on the physiological consequences of acute pain. Am J Hosp Pharm. 1994;51:1539–1554. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
