

Heart failure in North America
- PMID: 23597296
- PMCID: PMC3682397
- DOI: 10.2174/1573403x11309020006
Heart failure in North America
Abstract
Heart failure is a major health problem that affects patients and healthcare systems worldwide. Within the continent of North America, differences in economic development, genetic susceptibility, cultural practices, and trends in risk factors and treatment all contribute to both inter-continental and within-continent differences in heart failure. The United States and Canada represent industrialized countries with similar culture, geography, and advanced economies and infrastructure. During the epidemiologic transition from rural to industrial in countries such as the United States and Canada, nutritional deficiencies and infectious diseases made way for degenerative diseases such as cardiovascular diseases, cancer, overweight/obesity, and diabetes. This in turn has resulted in an increase in heart failure incidence in these countries, especially as overall life expectancy increases. Mexico, on the other hand, has a less developed economy and infrastructure, and has a wide distribution in the level of urbanization as it becomes more industrialized. Mexico is under a period of epidemiologic transition and the etiology and incidence of heart failure is rapidly changing. Ethnic differences within the populations of the United States and Canada highlight the changing demographics of each country as well as potential disparities in heart failure care. Heart failure with preserved ejection fraction makes up approximately half of all hospital admissions throughout North America; however, important differences in demographics and etiology exist between countries. Similarly, acute heart failure etiology, severity, and management differ between countries in North America. The overall economic burden of heart failure continues to be large and growing worldwide, with each country managing this burden differently. Understanding the inter-and within-continental differences may help improve understanding of the heart failure epidemic, and may aid healthcare systems in delivering better heart failure prevention and treatment.
Figures
References
-
- Yusuf S, Reddy S, Ounpuu S, Anand S. Global burden of cardiovascular diseases: part I: general considerations. the epidemiologic transition. risk factors. and impact of urbanization. Circulation. 2001;104(22):2746–53. - PubMed
-
- Reddy KS, Yusuf S. Emerging epidemic of cardiovascular disease in developing countries. Circulation. 1998;97(6):596–601. - PubMed
-
- Sen K, Bonita R. Global health status: two steps forward. one step back. Lancet. 2000;356(9229):577–82. - PubMed
-
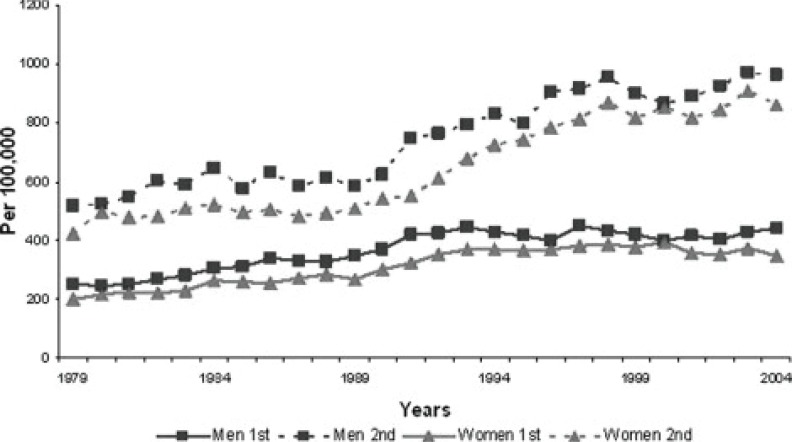
- Fang J, Mensah GA, Croft JB, Keenan NL. Heart failure-related hospitalization in the U. 1979 to 2004. J Am Coll Cardiol. 2008;52(6):428–34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
