

Cosmetic outcomes following head and neck melanoma reconstruction: The patient's perspective
- PMID: 23598768
- PMCID: PMC3307686
- DOI: 10.1177/229255031202000108
Cosmetic outcomes following head and neck melanoma reconstruction: The patient's perspective
Abstract
Background: While studies have compared aesthetic outcomes following wide local excision of head and neck melanoma, none have evaluated this important outcome from the patient's perspective. Indeed, one could argue that the psychosocial impact of head and neck melanoma excision and reconstruction is more accurately assessed by deriving patient-based as opposed to surgeon-based outcome measures.
Objective: To evaluate aesthetic outcomes following wide local excision of head and neck melanoma from the patient's perspective.
Methods: Fifty-one patients who underwent excision of 57 head and neck melanomas followed by immediate closure by primary repair, skin grafting, local flap coverage or free tissue transfer were asked to complete a written survey at least six months after their surgery. A visual analogue scale (VAS) was used to assess the patient's perception of appearance alteration, satisfaction with his or her appearance, and emotional impairment. An ordinal scale was used to evaluate several criteria of the reconstructive outcome (pain, itching, colour, scarring, stiffness, thickness and irregularity).
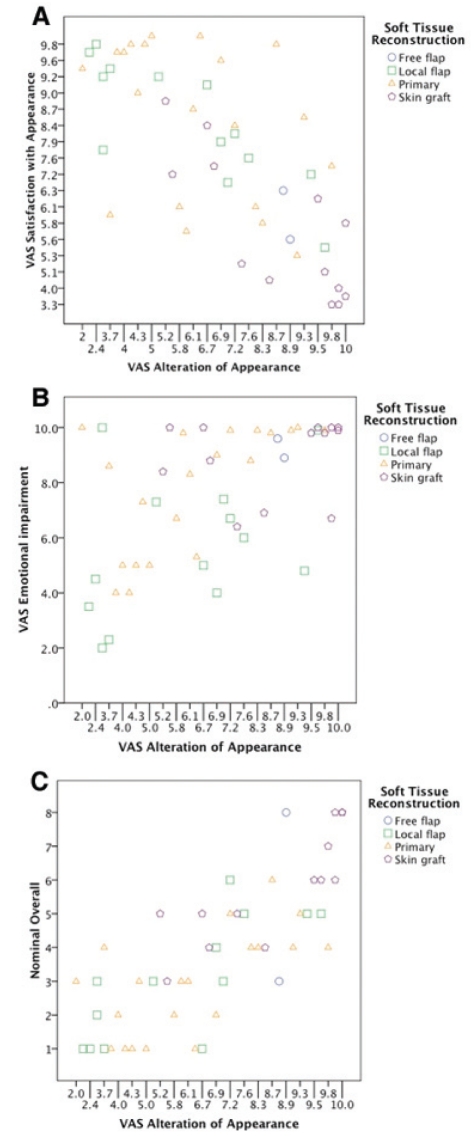
Results: Forty-two patients (82.4%) completed the survey. There were significant correlations between VAS scores reported for appearance alteration, satisfaction with outcome and emotional impairment (P=0.001). Patients who received skin grafts reported significantly unfavourable VAS scores compared with other methods of reconstruction (P=0.046). Moreover, skin grafts received significantly worse ordinal scale ratings for itching (P=0.043), colour (P=0.047), scarring (P=0.003) and stiffness (P=0.041) compared with other methods of reconstruction. Both skin grafts and free flaps were reported to have significantly less favourable thickness (P=0.012) and irregularity (P=0.036) than primary closure or local tissue transfer. There was no significant difference between patients undergoing primary closure with local tissue transfer (P>0.413). Other factors related to the patient's VAS scores included location of the melanoma (P=0.033), size of defect (P=0.037) and recurrence of melanoma (P=0.042).
Conclusion: The degree of emotional impairment following reconstruction of head and neck melanoma excision defects was correlated with the patient's perception of appearance alteration. From the patient's perspective, primary closure and local tissue transfer appeared to result in the highest aesthetic satisfaction.
Historique: Des études ont comparé les résultats esthétiques après une importante excision locale d’un mélanome de la tête et du cou, mais aucune ne s’est attardée sur ce résultat important selon le point de vue du patient. Pourtant, on peut faire valoir que les répercussions psychosociales de l’excision d’un mélanome de la tête et du cou seront évaluées de manière plus exacte d’après les mesures de résultats du patient que du chirurgien.
Objectif: Évaluer les résultats esthétiques après l’excision importante d’un mélanome de la tête et du cou selon le point de vue du patient.
Méthodologie: Cinquante et un patients qui ont subi une excision de 57 mélanomes de la tête et du cou suivie d’une fermeture immédiate par réparation primaire, par greffe cutanée, par recouvrement par un lambeau local ou par transfert de tissus libres ont été invités à répondre à un sondage écrit au moins six mois après l’opération. Une échelle analogique visuelle (ÉAV) a permis d’évaluer le point de vue du patient pour ce qui est de la modification de l’apparence, de la satisfaction envers l’apparence et de l’atteinte affective. Une échelle ordinale a servi à évaluer plusieurs critères des résultats de la reconstruction (douleur, démangeaison, couleur, cicatrice, épaisseur et irrégularité).
Résultats: Quarante-deux patients (82,4 %) ont répondu au sondage. Il y avait une importante corrélation entre les indices de l’ÉAV relatifs à la modification de l’apparence et à la satisfaction des résultats et celui de l’atteinte affective (P=0,001). Les patients qui avaient subi une greffe de la peau ont déclaré des indices d’ÉAV particulièrement défavorables par rapport à d’autres modes de reconstruction (P=0,046). De plus, les greffes cutanées ont reçu des résultats beaucoup plus négatifs à l’échelle ordinale relativement aux démangeaisons (P=0,043), à la couleur (P=0,047), aux cicatrices (P=0,003) et à la raideur (P=0,041) par rapport à d’autres modes de reconstruction. Tant les greffes cutanées que les lambeaux libres donnaient des résultats considérablement moins favorables sur le plan de l’épaisseur (P=0,012) et de l’irrégularité (P=0,036) que la fermeture primaire ou le transfert local de tissus. Il n’y avait pas de différence significative entre les patients qui subissaient une fermeture primaire par transfert local de tissus (P>0,413). D’autres facteurs liés aux indices d’ÉAV des patients incluaient l’emplacement du mélanome (P=0,033), la dimension de l’anomalie (P=0,037) et la récurrence du mélanome (P=0,042).
Conclusion: Le degré d’atteinte affective après la reconstruction d’anomalies causées par l’excision du mélanome de la tête et du cou était corrélé avec la perception qu’avait le patient des modifications à son apparence. Selon le point de vue du patient, la fermeture primaire et le transfert local de tissus semblaient s’associer à la plus grande satisfaction esthétique.
Keywords: Head and neck reconstruction; Local flap; Melanoma; Outcomes; Patient satisfaction.
Figures




Similar articles
-
The role of soft tissue reconstruction after melanoma resection in the head and neck.Head Neck. 2001 Jan;23(1):8-15. Head Neck. 2001. PMID: 11190860
-
The role of soft tissue reconstruction after melanoma resection in the head and neck.Head Neck. 2001 Jan;23(1):8-15. Head Neck. 2001. PMID: 11150065
-
Patient-Reported Aesthetic and Psychosocial Outcomes After Microvascular Reconstruction for Head and Neck Cancer.JAMA Otolaryngol Head Neck Surg. 2021 Dec 1;147(12):1035-1044. doi: 10.1001/jamaoto.2021.1563. JAMA Otolaryngol Head Neck Surg. 2021. PMID: 34292310 Free PMC article.
-
Recent advances in head and neck cancer reconstruction.Indian J Plast Surg. 2014 May;47(2):185-90. doi: 10.4103/0970-0358.138939. Indian J Plast Surg. 2014. PMID: 25190912 Free PMC article. Review.
-
Secondary Reconstruction of Head and Neck Cancer Defects-Principles in its Practice.J Maxillofac Oral Surg. 2023 Mar;22(Suppl 1):1-9. doi: 10.1007/s12663-023-01875-x. Epub 2023 Mar 2. J Maxillofac Oral Surg. 2023. PMID: 37041953 Free PMC article. Review.
Cited by
-
Beyond the Scalpel: Advancing Strategic Approaches and Targeted Therapies in Nonexcisable Melanomas.J Skin Cancer. 2024 Aug 27;2024:2167176. doi: 10.1155/2024/2167176. eCollection 2024. J Skin Cancer. 2024. PMID: 39229331 Free PMC article. Review.
-
Impact of Immediate Surgical Reconstruction Following Wide Local Excision of Malignant Head and Neck Melanoma.Plast Reconstr Surg Glob Open. 2020 Feb 24;8(2):e2661. doi: 10.1097/GOX.0000000000002661. eCollection 2020 Feb. Plast Reconstr Surg Glob Open. 2020. PMID: 32309102 Free PMC article.
-
Comparison of 1-cm Versus 2-cm Excision Margins for Cutaneous Melanoma: A Systematic Review and Meta-Analysis.Cureus. 2025 May 26;17(5):e84848. doi: 10.7759/cureus.84848. eCollection 2025 May. Cureus. 2025. PMID: 40568274 Free PMC article. Review.
-
Reading Between the Lines: A Five-Point Narrative Approach to Online Accounts of Illness.J Med Humanit. 2019 Dec;40(4):569-590. doi: 10.1007/s10912-019-09553-1. J Med Humanit. 2019. PMID: 30982939 Free PMC article.
-
An organizational framework for patient-reported outcome instruments in dermatologic surgery: a systematic review and qualitative analysis.Arch Dermatol Res. 2023 Dec 4;316(1):15. doi: 10.1007/s00403-023-02738-8. Arch Dermatol Res. 2023. PMID: 38047921
References
-
- Fisher SR, O’Brien CJ. Head and neck melanoma. In: Balch CM, Houghton AN, Sober AJ, Hoong S, editors. Cutaneous Melanoma. St Louis: Quality Medical Publishing, Inc; 1998. pp. 163–71.
-
- Brown TJ, Nelson BR. Malignant melanoma: A clinical review. Cutis. 1999;63:275–8. 281–4. - PubMed
-
- Coit DG. NCCN Practice Guidelines in Oncology- v.2.2009: Melanoma. National Comprehensive Cancer Network. < www.nccn.org> Last accessed February 19, 2009.
-
- Bogle M, Kelly P, Shenaq J, Friedman J, Evans G. The role of soft tissue reconstruction after melanoma resection in the head and neck. Head Neck. 2001;23:8–15. - PubMed
-
- Eshima I. The role of plastic surgery in the treatment of malignant melanoma. Surg Clin North Am. 1996;76:1331–42. - PubMed
LinkOut - more resources
Full Text Sources