

Peripheral T-cell lymphomas of follicular T-helper cell derivation with Hodgkin/Reed-Sternberg cells of B-cell lineage: both EBV-positive and EBV-negative variants exist
- PMID: 23598959
- PMCID: PMC3654051
- DOI: 10.1097/PAS.0b013e3182785610
Peripheral T-cell lymphomas of follicular T-helper cell derivation with Hodgkin/Reed-Sternberg cells of B-cell lineage: both EBV-positive and EBV-negative variants exist
Abstract
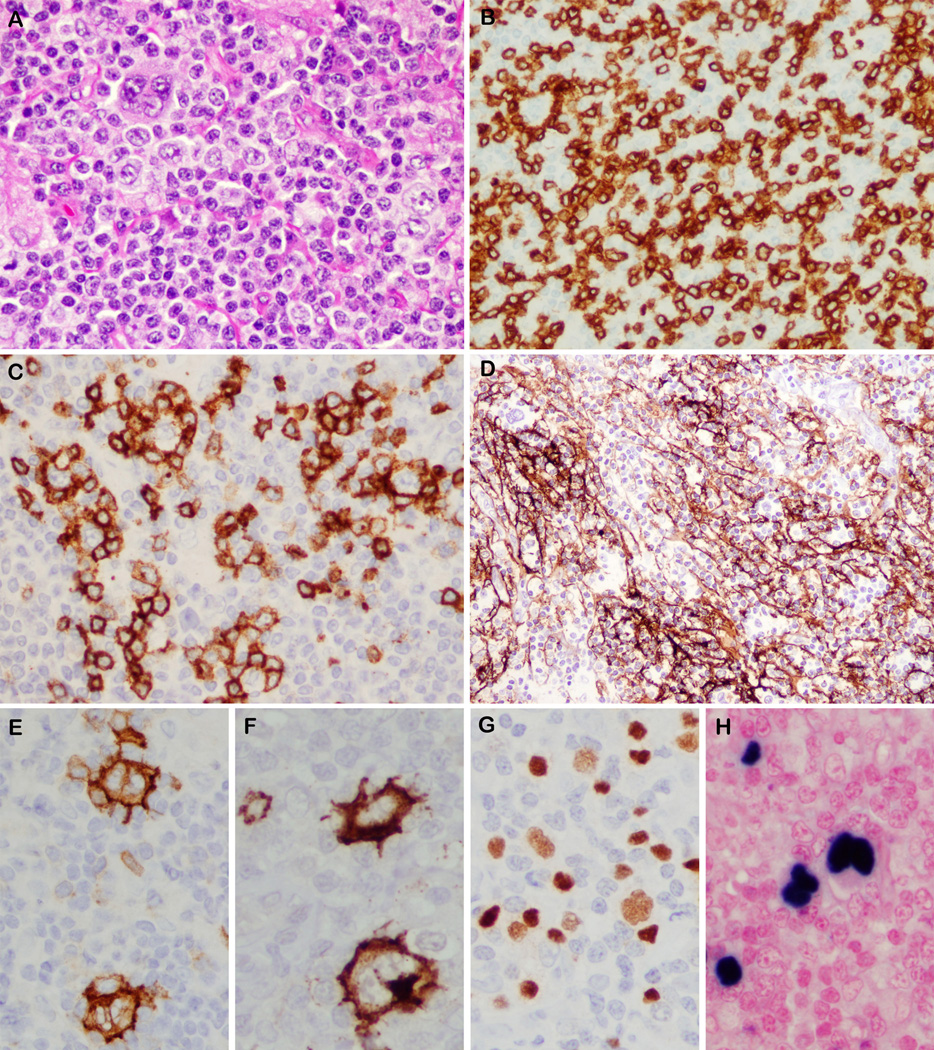
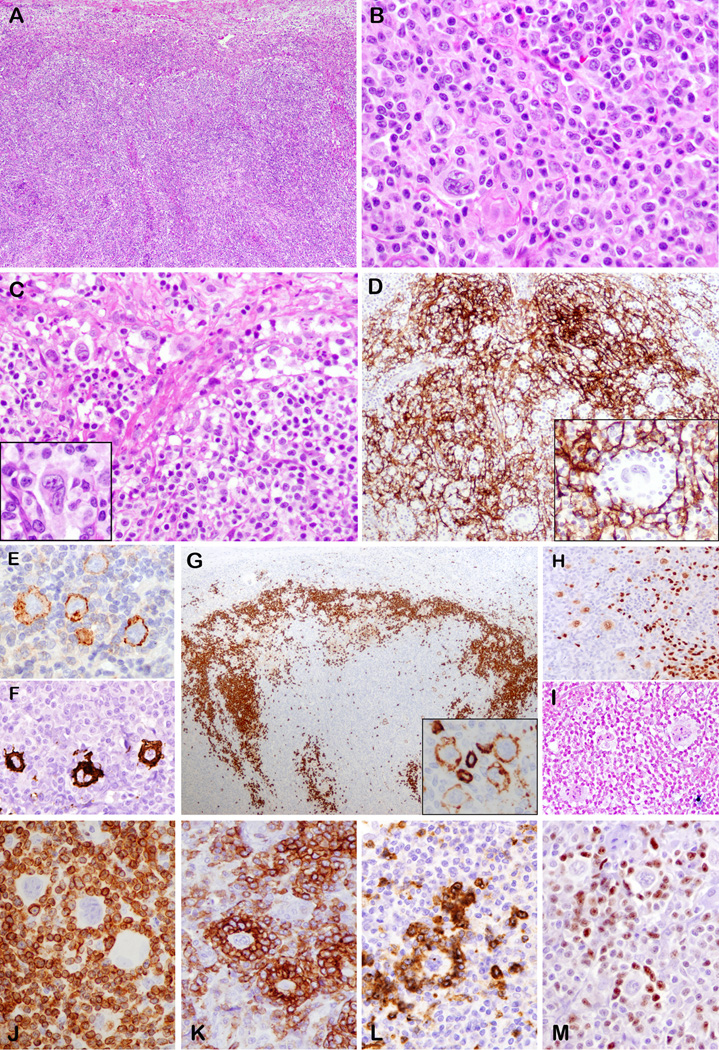
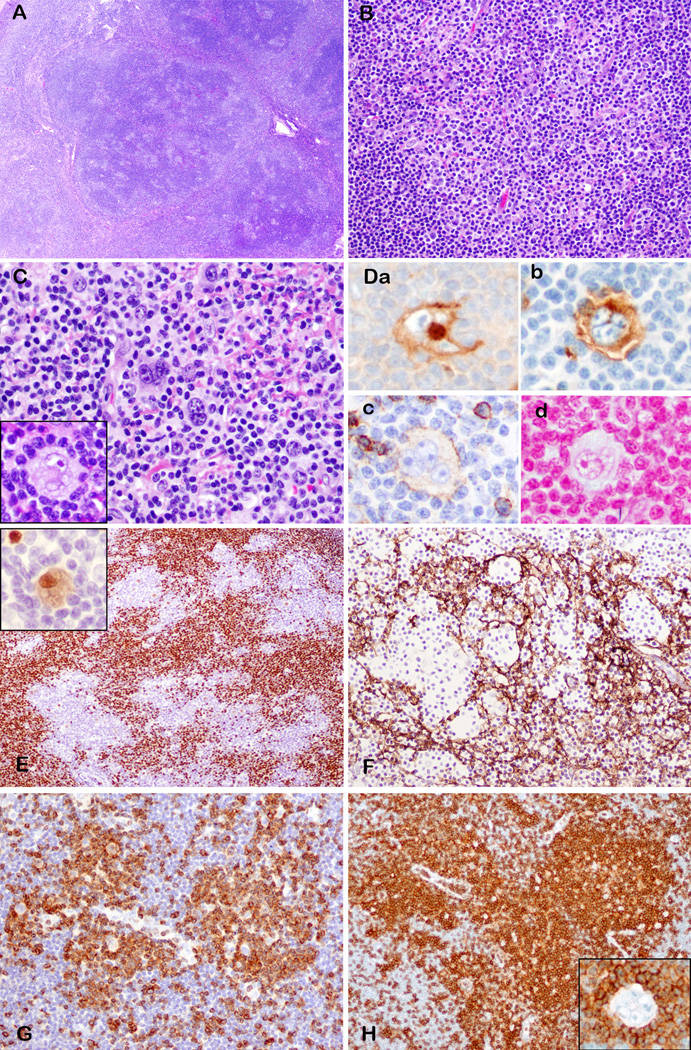
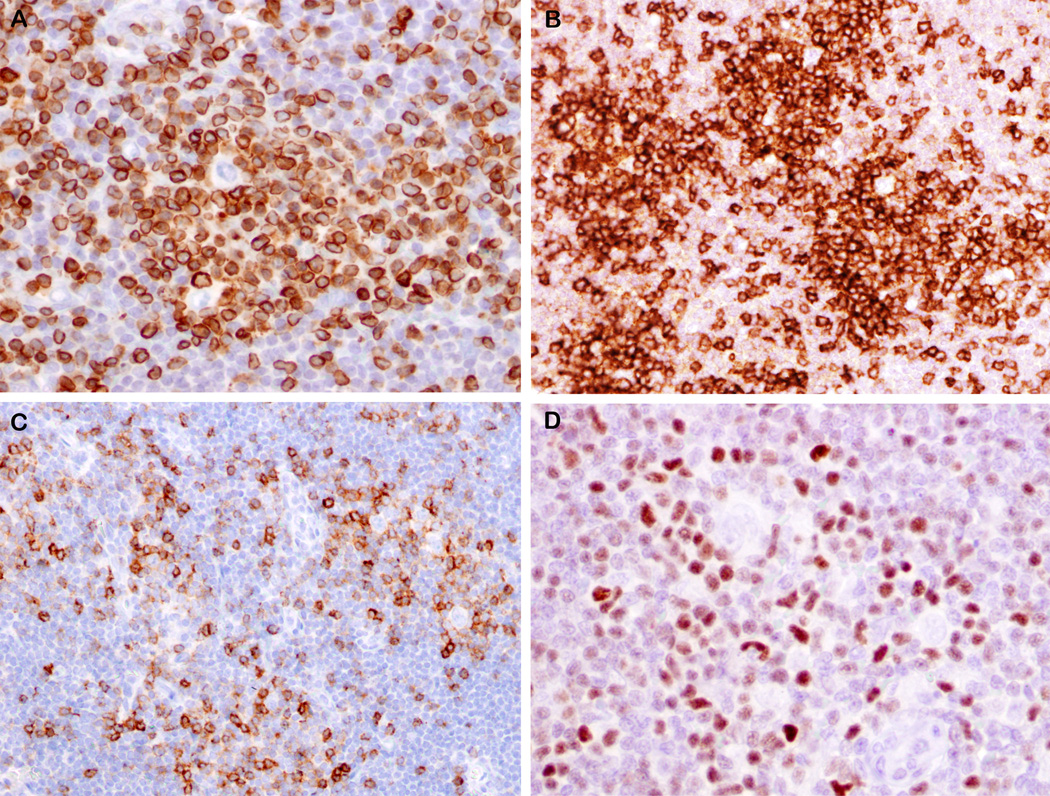
Peripheral T-cell lymphomas (PTCLs) are functionally and morphologically complex. Epstein-Barr virus (EBV)-positive B cells have been reported in angioimmunoblastic T-cell lymphoma (AITL) and other PTCLs and may mimic Hodgkin/Reed-Sternberg (HRS) cells, but EBV-negative HRS-like B cells have not been described. We wished to assess the nature of the PTCL associated with HRS-like cells and to determine whether EBV-negative HRS-like cells may be seen. We identified 57 PTCL cases reported as containing HRS-like cells. These included 32 AITL, 19 PTCL, not otherwise specified (NOS), 3 PTCL-NOS, follicular variant, 1 PTCL-NOS, T-zone variant, and 2 adult T-cell leukemia/lymphoma cases. All patients were adults with a median age of 63 and presented with lymphadenopathy. The male:female ratio was 31:26 (1.2:1). Clonal TRG rearrangement was detected in 46/53 cases. Six of 38 cases had a concomitant clonal immunoglobulin gene rearrangement. In 52/57 cases the HRS cells were positive for EBV. Five cases, 3 classified as AITL and 2 as PTCL-NOS, follicular variant, contained HRS-like cells negative for EBV. All PTCLs with EBV-negative HRS cells had a T follicular helper cell immunophenotype. The neoplastic T cells expressed CD3, CD4, and PD-1 and formed rosettes around the HRS-like cells. The HRS-like cells were positive for CD20 (variable intensity), PAX5, CD30, and CD15 (4/5). We conclude that both EBV-positive and EBV-negative HRS-like B cells may occur in the background of PTCL; caution is needed to avoid misdiagnosis as classical Hodgkin lymphoma. The close interaction between the HRS-like cells and the rosetting PD-1-positive T cells suggests a possible pathogenetic role in this phenomenon and provides new insights into the abnormal B-cell proliferations that occur in the context of TFH malignancies.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Clinicopathological Study of 30 Cases of Peripheral T-cell Lymphoma with Hodgkin and Reed-Sternberg-like B-cells from Japan.Am J Surg Pathol. 2017 Apr;41(4):506-516. doi: 10.1097/PAS.0000000000000813. Am J Surg Pathol. 2017. PMID: 28125450
-
Peripheral T-cell lymphoma with Reed-Sternberg-like cells of B-cell phenotype and genotype associated with Epstein-Barr virus infection.Am J Surg Pathol. 1999 Oct;23(10):1233-40. doi: 10.1097/00000478-199910000-00008. Am J Surg Pathol. 1999. PMID: 10524524
-
Follicular peripheral T-cell lymphoma expands the spectrum of classical Hodgkin lymphoma mimics.Am J Surg Pathol. 2012 Nov;36(11):1636-46. doi: 10.1097/PAS.0b013e318268d9ff. Am J Surg Pathol. 2012. PMID: 23073322
-
Follicular helper T-cell lymphomas: disease spectrum, relationship with clonal hematopoiesis, and mimics. A report of the 2022 EA4HP/SH lymphoma workshop.Virchows Arch. 2023 Sep;483(3):349-365. doi: 10.1007/s00428-023-03607-5. Epub 2023 Jul 27. Virchows Arch. 2023. PMID: 37500795 Free PMC article. Review.
-
Primary extranodal soft tissue Lennert lymphoma (lymphoepithelioid variant of peripheral T-cell lymphoma, unspecified): a case report and review of the literature.Diagn Pathol. 2023 Feb 3;18(1):12. doi: 10.1186/s13000-023-01297-w. Diagn Pathol. 2023. PMID: 36737805 Free PMC article. Review.
Cited by
-
Advances in understanding of angioimmunoblastic T-cell lymphoma.Leukemia. 2020 Oct;34(10):2592-2606. doi: 10.1038/s41375-020-0990-y. Epub 2020 Jul 23. Leukemia. 2020. PMID: 32704161 Free PMC article. Review.
-
Prognostic significance of CD30 expression in nasal natural killer/T-cell lymphoma.Oncol Lett. 2017 Mar;13(3):1211-1215. doi: 10.3892/ol.2017.5592. Epub 2017 Jan 11. Oncol Lett. 2017. PMID: 28454236 Free PMC article.
-
Pathobiology of T-cell and NK-cell lymphomas.Best Pract Res Clin Haematol. 2013 Mar;26(1):75-87. doi: 10.1016/j.beha.2013.04.007. Epub 2013 May 23. Best Pract Res Clin Haematol. 2013. PMID: 23768642 Free PMC article. Review.
-
MUM-1 expression differentiates AITL with HRS-like cells from cHL.Int J Clin Exp Pathol. 2015 Sep 1;8(9):11372-8. eCollection 2015. Int J Clin Exp Pathol. 2015. PMID: 26617862 Free PMC article.
-
A practical approach to the modern diagnosis and classification of T- and NK-cell lymphomas.Blood. 2024 Oct 31;144(18):1855-1872. doi: 10.1182/blood.2023021786. Blood. 2024. PMID: 38728419 Review.
References
-
- Abruzzo LV, Schmidt K, Weiss LM, et al. B-cell lymphoma after angioimmunoblastic lymphadenopathy: a case with oligoclonal gene rearrangements associated with Epstein-Barr virus. Blood. 1993;82:241–246. - PubMed
-
- Higgins JP, van de Rijn M, Jones CD, Zehnder JL, Warnke RA. Peripheral T-cell lymphoma complicated by a proliferation of large B cells. Am J Clin Pathol. 2000;114:236–247. - PubMed
-
- Zettl A, Lee SS, Rudiger T, et al. Epstein-Barr virus-associated B-cell lymphoproliferative disorders in angloimmunoblastic T-cell lymphoma and peripheral T-cell lymphoma, unspecified. Am J Clin Pathol. 2002;117:368–379. - PubMed
-
- Attygalle AD, Kyriakou C, Dupuis J, et al. Histologic evolution of angioimmunoblastic T-cell lymphoma in consecutive biopsies: clinical correlation and insights into natural history and disease progression. Am J Surg Pathol. 2007;31:1077–1088. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
