

Comparison of WHO Classifications (2004, 2010), the Hochwald grading system, and AJCC and ENETS staging systems in predicting prognosis in locoregional well-differentiated pancreatic neuroendocrine tumors
- PMID: 23598967
- PMCID: PMC3654011
- DOI: 10.1097/PAS.0b013e31827fcc18
Comparison of WHO Classifications (2004, 2010), the Hochwald grading system, and AJCC and ENETS staging systems in predicting prognosis in locoregional well-differentiated pancreatic neuroendocrine tumors
Abstract
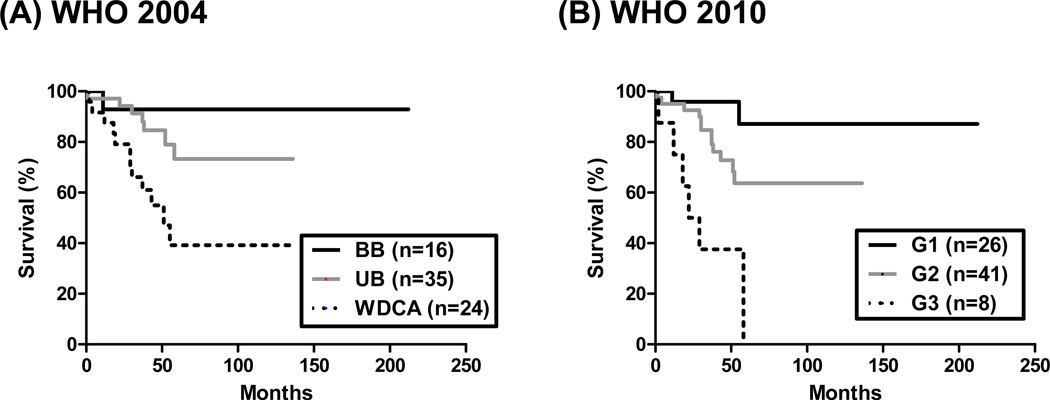
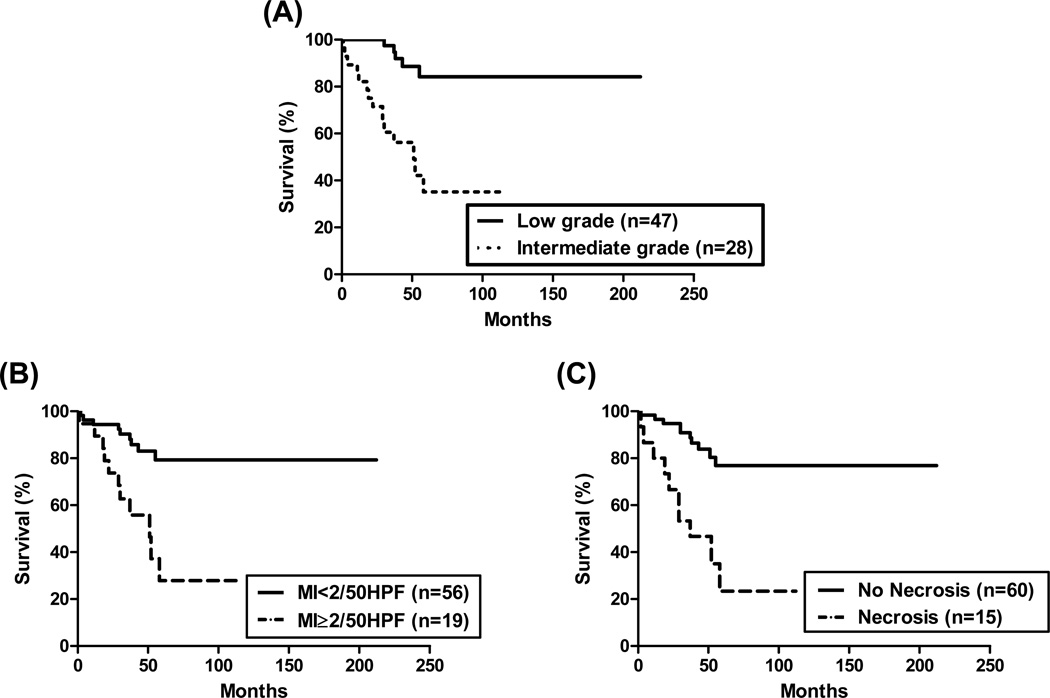
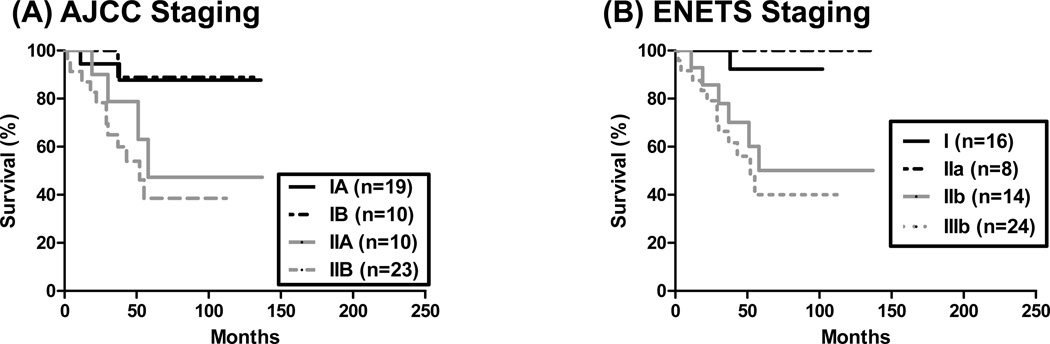
It is difficult to predict prognosis in patients with locoregional well-differentiated (WD) pancreatic neuroendocrine tumors (PanNET). We aimed to examine commonly used stratification systems [World Health organization (WHO) 2004 and 2010 classifications, American Joint Committee on Cancer (AJCC) and European Neuroendocrine Tumor Society (ENETS) staging, and the Hochwald grading system] for their power in predicting recurrence-free survival (RFS) in these patients. Seventy-five such patients (mean age 56 y, mean follow-up 79 mo) who underwent resection with sufficient tissue material and follow-up data were studied. RFS was correlated with variable clinicopathologic features and stratified with above-mentioned systems. Concordance index (CI) was then calculated. With the WHO 2004 classification, 16, 35, and 24 PanNETs were classified as benign behavior, uncertain behavior, and WD endocrine carcinoma, respectively. By the WHO 2010 classification, 26, 41, and 8 tumors were grade 1, 2, and 3, respectively. Using the Hochwald system, 47 were low grade, and 28 were intermediate grade. The AJCC staging information was complete for 62 patients (13 had the lymph node status Nx) and included: stages IA (19/62), IB (10/62), IIA (10/62), and IIB (23/62). The ENETS staging information was stages I (16/62), IIa (8/62), IIb (14/62), IIIa (0/62), and IIIb (24/62). The average Ki-67 proliferation index (PI) was 8.1%. Factors that predicted RFS included tumor size, nodal metastasis, vascular invasion, perineural invasion, necrosis, mitosis, and Ki-67 PI (all P<0.01). The CI for each system was: 0.6361 for WHO 2004, 0.6735 for WHO 2010, 0.6495 for AJCC staging, 0.6642 for ENETS staging, and 0.6851 for the Hochwald grading system. When these systems were analyzed in conjunction with various additional important pathologic features, combination of the Hochwald grading system and Ki-67 PI achieved the highest CI (0.7946). Therefore, although all these systems predict RFS well in locoregional WD PanNETs, the Hochwald grading system achieves the highest predictive ability. Further predictive power can be achieved by combining the Hochwald grading system and Ki-67 PI.
Conflict of interest statement
Figures
References
-
- Klimstra DS, Modlin IR, Coppola D, et al. The pathologic classification of neuroendocrine tumors: a review of nomenclature, grading, and staging systems. Pancreas. 2010;39:707–712. - PubMed
-
- Hochwald SN, Zee S, Conlon KC, et al. Prognostic factors in pancreatic endocrine neoplasms: an analysis of 136 cases with a proposal for low-grade and intermediate-grade groups. J Clin Oncol. 2002;20:2633–2642. - PubMed
-
- Klimstra DS, Arnold R, Capella C, et al. WHO Classification of Tumours of the Digestive System. In: Bosman FT, Carneiro F, Hruban RH, Theise ND, editors. Tumours of the pancreas. Lyon: International Agency for Research on Cancer (IARC); 2010. pp. 279–337.
-
- Exocrine and endocrine pancreas. New York, NY: Springer; 2010. AJCC Cancer Staging Manual; pp. 241–249.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
