

Minimal access median sternotomy for aortic valve replacement in elderly patients
- PMID: 23601376
- PMCID: PMC3652735
- DOI: 10.1186/1749-8090-8-103
Minimal access median sternotomy for aortic valve replacement in elderly patients
Abstract
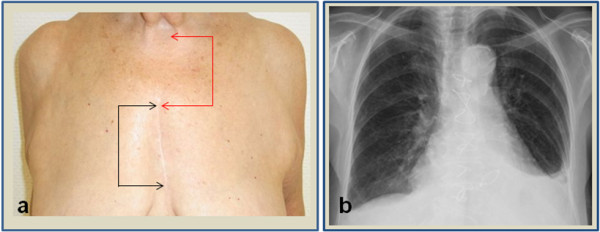
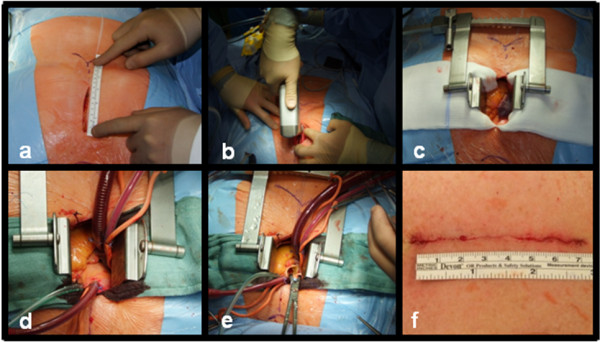
Background: We report our clinical experience with a approach for aortic valve replacement (AVR) via minimal access skin incision and complete median sternotomy. This approach was used in patients with higher age and multiple co-morbidities, facilitating an easy access with short bypass and cross clamp times. It was especially performed in patients asking for an excellent cosmetic result, who did not qualifying for minimally-invasive AVR via partial upper sternotomy.
Methods: AVR via minimal-access median sternotomy, was performed in 58 patients between 01/2009 and 11/2011. Intra- and postoperative data including cross clamp time, cardiopulmonary bypass time, mortality, stroke, pacemaker implantation, re-operation for bleeding, ventilation time, ICU and hospital stay, wound infection, sternal dehiscence or fracture and 30 day mortality were collected.
Results: Mean patients age was 76.1 +/-9.4 years, 72% were female. Minimal-access AVR could be performed with a mean length of midline skin incision of 7.8 cm. Aortic cross-clamping time was 54.6 +/-6.3 min, cardiopulmonary bypass time 71.2+/-11.3 min and time of surgery 154.1 +/-26.8 min. Re-operation for bleeding had to be performed in 1 case (1.7%). There were no strokes or pacemaker implantations needed. Mean ventilation time was 4.5 h, ICU stay was 2 days and mean length of hospital stay was 6 days. 6 months follow up showed mortality of 0% and no sternal dehiscence or wound infection was observed.
Conclusion: Minimal-access AVR via complete median sternotomy can be performed safely,in this elderly patient cohort without adding additional operative risk compared to conventional AVR. By avoidiance of large skin incisions this approach combines excellent cosmetic results with fast surgery time and excellent postoperative recovery.
Figures
Similar articles
-
Benefits of rapid deployment aortic valve replacement with a mini upper sternotomy.J Cardiothorac Surg. 2020 Aug 26;15(1):226. doi: 10.1186/s13019-020-01268-y. J Cardiothorac Surg. 2020. PMID: 32847577 Free PMC article.
-
Is the femoral cannulation for minimally invasive aortic valve replacement necessary?Eur J Cardiothorac Surg. 1998 Oct;14 Suppl 1:S111-4. doi: 10.1016/s1010-7940(98)00116-x. Eur J Cardiothorac Surg. 1998. PMID: 9814804
-
Partial upper re-sternotomy for aortic valve replacement or re-replacement after previous cardiac surgery.Eur J Cardiothorac Surg. 2000 Sep;18(3):282-6. doi: 10.1016/s1010-7940(00)00528-5. Eur J Cardiothorac Surg. 2000. PMID: 10973536
-
Minimally Invasive Aortic Valve Replacement: Cost-Benefit Analysis of Ministernotomy Versus Minithoracotomy Approach.J Heart Valve Dis. 2015 Sep;24(5):531-9. J Heart Valve Dis. 2015. PMID: 26897831 Review.
-
Mini-sternotomy vs right anterior thoracotomy for aortic valve replacement.J Card Surg. 2020 Jul;35(7):1570-1582. doi: 10.1111/jocs.14607. J Card Surg. 2020. PMID: 32652784
Cited by
-
Aortic Valve Replacement: Treatment by Sternotomy versus Minimally Invasive Approach.Braz J Cardiovasc Surg. 2016 Nov-Dec;31(6):422-427. doi: 10.5935/1678-9741.20160085. Braz J Cardiovasc Surg. 2016. PMID: 28076618 Free PMC article.
-
Influence of body mass index on outcomes after minimal-access aortic valve replacement through a J-shaped partial upper sternotomy.J Cardiothorac Surg. 2016 Apr 27;11(1):74. doi: 10.1186/s13019-016-0467-2. J Cardiothorac Surg. 2016. PMID: 27118140 Free PMC article.
-
Minimally invasive aortic valve replacement in high risk patient groups.J Thorac Dis. 2017 Jun;9(6):1672-1696. doi: 10.21037/jtd.2017.05.21. J Thorac Dis. 2017. PMID: 28740685 Free PMC article. Review.
-
Minimal access aortic valve replacement via limited skin incision and complete median sternotomy.J Thorac Dis. 2013 Nov;5 Suppl 6(Suppl 6):S654-7. doi: 10.3978/j.issn.2072-1439.2013.09.23. J Thorac Dis. 2013. PMID: 24251023 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
