

Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA study): overall survival results from a randomised, double-blind, placebo-controlled, phase 3 study
- PMID: 23602601
- PMCID: PMC4076842
- DOI: 10.1016/S1470-2045(13)70130-X
Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA study): overall survival results from a randomised, double-blind, placebo-controlled, phase 3 study
Abstract
Background: CLEOPATRA is a phase 3 study to compare the efficacy and safety of pertuzumab, trastuzumab, and docetaxel with placebo, trastuzumab, and docetaxel in patients with HER2-positive first-line metastatic breast cancer. The results of the primary analysis showed significantly longer median progression-free survival in the pertuzumab group than in the placebo group. Interim analysis of overall survival favoured the pertuzumab group but was not significant. Here, we report results for overall survival after an additional year of follow-up.
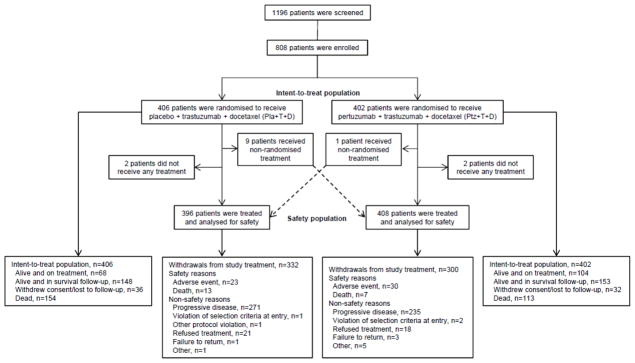
Methods: The study was a double-blind randomised trial undertaken at 204 centres in 25 countries. Patients with HER2-positive metastatic breast cancer who had not received previous chemotherapy or biological treatment for their metastatic disease were randomly assigned to receive either pertuzumab, trastuzumab, and docetaxel (n=402) or the same regimen with a matching placebo replacing pertuzumab (n=406). Randomisation was in a 1:1 ratio, stratified by geographical region and previous treatment status. The primary endpoint was progression-free survival (assessed independently), which has been reported previously; no follow-up data were gathered for the primary endpoint. Secondary endpoints included overall survival, progression-free survival (assessed by investigator), objective response rate, and safety. Median follow-up was 30 months in both groups. Efficacy endpoints were analysed in the intention-to-treat population and safety was analysed by treatment received. The study is completed but safety and survival data continue to be followed up. This trial is registered with ClinicalTrials.gov, number NCT00567190.
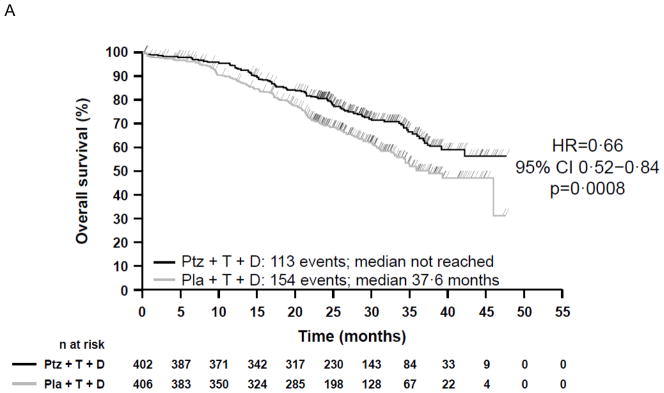
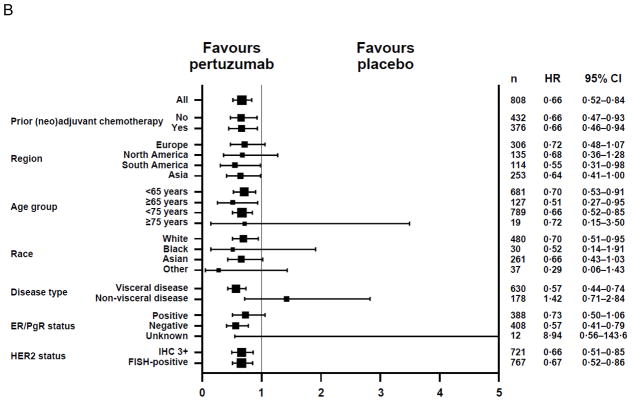
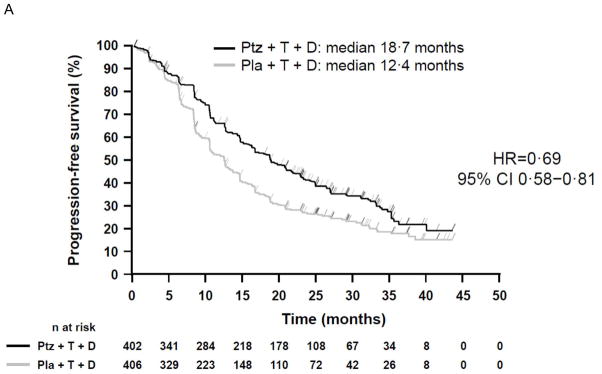
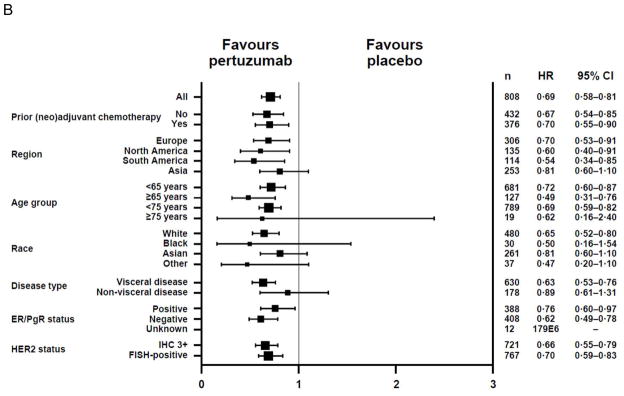
Findings: In the intention-to-treat population, 267 patients died by data cutoff (May 14, 2012), 154 (38%) of 406 in the placebo group and 113 (28%) of 402 in the pertuzumab group. Median overall survival was 37.6 months (95% CI 34.3-NE [not estimable]) in the placebo group but had not been reached (95% CI 42.4-NE) in the pertuzumab group (hazard ratio 0.66, 95% CI 0.52-0.84; p=0.0008). Investigator-assessed median progression-free survival was 12.4 months (95% CI 10.4-13.5) in the placebo group and 18.7 months (16.6-21.6) in the pertuzumab group (hazard ratio 0.69, 95% CI 0.58-0.81). Serious adverse events were reported in 115 (29%) of 396 patients who received placebo, trastuzumab, and docetaxel and 148 (36%) of 408 who received pertuzumab, trastuzumab, and docetaxel, and included febrile neutropenia, neutropenia, diarrhoea, pneumonia, and cellulitis. Overall, adverse events were similar to those reported at the primary analysis with respect to frequency, severity, and specificity.
Interpretation: Our analysis shows a significant improvement in overall survival with pertuzumab, trastuzumab, and docetaxel in patients with HER2-positive metastatic breast cancer, compared with placebo, trastuzumab, and docetaxel. Since this effect was not achieved at the expense of adverse events, this regimen represents a substantial improvement on the standard of care for this population of patients.
Funding: F Hoffmann-La Roche, Genentech.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Conflict of interest statement
SMS discloses an uncompensated consultant/advisory role for Roche/Genentech; her institution has received research funding from Roche/Genentech, Agendia, and Pfizer/PUMA. JC is a consultant for Roche, Celgene, and Novartis and has received honoraria from Roche, Celgene, Novartis, and Eisai. J-MF has received honoraria from Roche, Pfizer, and Sanofi-Aventis. AS is a consultant for Roche and Sanofi-Aventis and has received honoraria from both companies. AK, ECl, and GR are employees of Roche Products Limited. ECl discloses stock ownership from AstraZeneca. GR discloses stock ownership from Roche and GlaxoSmithKline; an immediate family member owns stocks from GlaxoSmithKline. MCB is an employee of Genentech. JB discloses a consultant/advisory role for Roche/Genentech and Sanofi-Aventis. S-BK, JR, VS, MC, and ECi have no conflicts of interest to disclose.
Figures
Comment in
-
Targeted treatments for breast cancer: a step forward.Lancet Oncol. 2013 May;14(6):438-9. doi: 10.1016/S1470-2045(13)70153-0. Epub 2013 Apr 18. Lancet Oncol. 2013. PMID: 23602602 No abstract available.
References
-
- Ross JS, Slodkowska EA, Symmans WF, Pusztai L, Ravdin PM, Hortobagyi GN. The HER-2 receptor and breast cancer: ten years of targeted anti-HER-2 therapy and personalized medicine. Oncologist. 2009;14(4):320–68. - PubMed
-
- Wolff AC, Hammond ME, Schwartz JN, Hagerty KL, Allred DC, Cote RJ, et al. American Society of Clinical Oncology/College of American Pathologists Guideline Recommendations for Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer. Arch Pathol Lab Med. 2007;131(1):18–43. - PubMed
-
- Slamon DJ, Leyland-Jones B, Shak S, Fuchs H, Paton V, Bajamonde A, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001;344(11):783–92. - PubMed
-
- Marty M, Cognetti F, Maraninchi D, Snyder R, Mauriac L, Tubiana-Hulin M, et al. Randomized phase II trial of the efficacy and safety of trastuzumab combined with docetaxel in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer administered as first-line treatment: the M77001 study group. J Clin Oncol. 2005;23(19):4265–74. - PubMed
Appendix
References used for systematic review
-
- Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001;344:783–92. - PubMed
-
- Andersson M, Lidbrink E, Bjerre K, et al. Phase III randomized study comparing docetaxel plus trastuzumab with vinorelbine plus trastuzumab as first-line therapy of metastatic or locally advanced human epidermal growth factor receptor 2-positive breast cancer: the HERNATA study. J Clin Oncol. 2011;29:264–71. - PubMed
-
- Valero V, Forbes J, Pegram MD, et al. Multicenter phase III randomized trial comparing docetaxel and trastuzumab with docetaxel, carboplatin, and trastuzumab as first-line chemotherapy for patients with HER2-gene-amplified metastatic breast cancer (BCIRG 007 study): two highly active therapeutic regimens. J Clin Oncol. 2011;29:149–56. - PubMed
-
- Marty M, Cognetti F, Maraninchi D, et al. Randomized phase II trial of the efficacy and safety of trastuzumab combined with docetaxel in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer administered as first-line treatment: the M77001 study group. J Clin Oncol. 2005;23:4265–74. - PubMed
-
- Ardavanis A, Tryfonopoulos D, Orfanos G, et al. Safety and efficacy of trastuzumab every 3 weeks combined with cytotoxic chemotherapy in patients with HER2-positive recurrent breast cancer: findings from a case series. Onkologie. 2005;28:558–64. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
