

Radiochemotherapy plus 3-aminopyridine-2-carboxaldehyde thiosemicarbazone (3-AP, NSC #663249) in advanced-stage cervical and vaginal cancers
- PMID: 23603372
- PMCID: PMC4260802
- DOI: 10.1016/j.ygyno.2013.04.019
Radiochemotherapy plus 3-aminopyridine-2-carboxaldehyde thiosemicarbazone (3-AP, NSC #663249) in advanced-stage cervical and vaginal cancers
Abstract
Objective: Cervical and vaginal cancers have virally-mediated or mutated defects in DNA damage repair responses, making these cancers sensible targets for ribonucleotide reductase inhibition during radiochemotherapy.
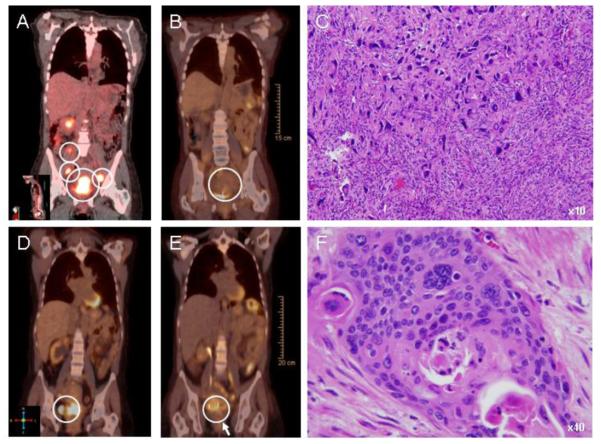
Methods: We conducted a phase II study evaluating 3× weekly 2-hour intravenous 3-aminopyridine-2-carboxaldehyde thiosemicarbazone (3-AP, 25 mg/m(2)) co-administered with 1× weekly intravenous cisplatin (40 mg/m(2)) and daily pelvic radiation (45 Gy) in women with stage I(B2)-IV(B) cervical (n=22) or stage II-IV vaginal (n=3) cancers. Brachytherapy followed (40 Gy). Toxicity was monitored by common terminology criteria for adverse events (version 3.0). The primary end point of response was assessed by 3-month posttherapy 2-[(18)F] fluoro-2-deoxy-d-glucose positron emission tomography (PET/CT) and clinical examination.
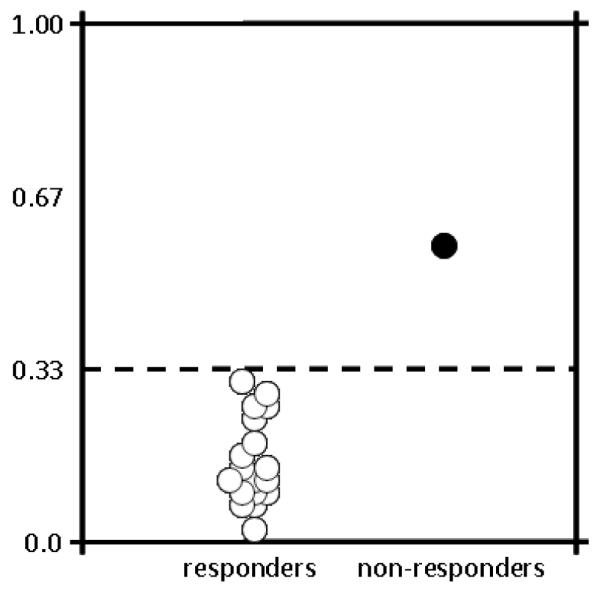
Results: 3-AP radiochemotherapy achieved clinical responses in 24 (96% [95% confidence interval: 80-99%]) of 25 patients (median follow-up 20 months, range 2-35 months). 23 (96% [95% confidence interval: 80-99%]) of 24 patients had 3-month posttherapy PET/CT scans that recorded metabolic activity in the cervix or vagina equal or less than that of the cardiac blood pool, suggesting complete metabolic responses. The most frequent 3-AP radiochemotherapy-related adverse events included fatigue, nausea, diarrhea, and reversible hematological and electrolyte abnormalities.
Conclusions: The addition of 3-AP to cisplatin radiochemotherapy was tolerable and produced high rates of clinical and metabolic responses in women with cervical and vaginal cancers. Future randomized phase II and III clinical trials of 3-AP radiochemotherapy are warranted.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
References
-
- Rose P, Ali S, Watkins E, Thigpen J, Deppe G, Clark-Pearson D, et al. Long-term follow-up of a randomized trial comparing concurrent single agent cisplatin, cisplatin-based combination chemotherapy, or hydroxyurea during pelvic irradiation for locally advanced cervical cancer: A Gynecologic Oncology Group Study. J Clin Oncol. 2007;25:2804–10. - PubMed
-
- Kunos C, Radivoyevitch T, Abdul-Karim F, Faulhaber P. 18F-fluoro-2-deoxy-d-glucose positron emission tomography standard uptake value as an indicator of cervical cancer chemoradiation therapeutic response. Int J Gynecol Cancer. 2011;21:1117–23. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
