

Expiratory flow limitation definition, mechanisms, methods, and significance
- PMID: 23606962
- PMCID: PMC3625607
- DOI: 10.1155/2013/749860
Expiratory flow limitation definition, mechanisms, methods, and significance
Abstract
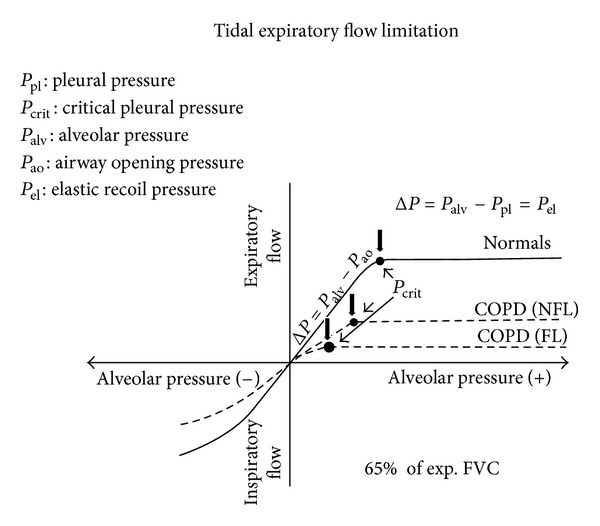
When expiratory flow is maximal during tidal breathing and cannot be increased unless operative lung volumes move towards total lung capacity, tidal expiratory flow limitation (EFL) is said to occur. EFL represents a severe mechanical constraint caused by different mechanisms and observed in different conditions, but it is more relevant in terms of prevalence and negative consequences in obstructive lung diseases and particularly in chronic obstructive pulmonary disease (COPD). Although in COPD patients EFL more commonly develops during exercise, in more advanced disorder it can be present at rest, before in supine position, and then in seated-sitting position. In any circumstances EFL predisposes to pulmonary dynamic hyperinflation and its unfavorable effects such as increased elastic work of breathing, inspiratory muscles dysfunction, and progressive neuroventilatory dissociation, leading to reduced exercise tolerance, marked breathlessness during effort, and severe chronic dyspnea.
Figures


Similar articles
-
Dyspnea During Night-Time and at Early Morning in Patients with Stable COPD is Associated with Supine Tidal Expiratory Flow Limitation.Int J Chron Obstruct Pulmon Dis. 2020 Oct 16;15:2549-2558. doi: 10.2147/COPD.S269346. eCollection 2020. Int J Chron Obstruct Pulmon Dis. 2020. PMID: 33116471 Free PMC article.
-
Flow limitation: an overview.Monaldi Arch Chest Dis. 1999 Aug;54(4):353-7. Monaldi Arch Chest Dis. 1999. PMID: 10546481 Review.
-
Expiratory flow limitation and orthopnea in massively obese subjects.Chest. 2001 May;119(5):1401-8. doi: 10.1378/chest.119.5.1401. Chest. 2001. PMID: 11348945
-
Volume effect and exertional dyspnoea after bronchodilator in patients with COPD with and without expiratory flow limitation at rest.Thorax. 2002 Jun;57(6):528-32. doi: 10.1136/thorax.57.6.528. Thorax. 2002. PMID: 12037229 Free PMC article.
-
Physiological techniques for detecting expiratory flow limitation during tidal breathing.Eur Respir Rev. 2011 Sep 1;20(121):147-55. doi: 10.1183/09059180.00001911. Eur Respir Rev. 2011. PMID: 21881143 Free PMC article. Review.
Cited by
-
Nasal high-flow bronchodilator nebulization: a randomized cross-over study.Ann Intensive Care. 2018 Dec 20;8(1):128. doi: 10.1186/s13613-018-0473-8. Ann Intensive Care. 2018. PMID: 30570679 Free PMC article.
-
Exertional dyspnoea in obesity.Eur Respir Rev. 2016 Dec;25(142):487-495. doi: 10.1183/16000617.0081-2016. Eur Respir Rev. 2016. PMID: 27903669 Free PMC article. Review.
-
Effect of body position on peak expiratory flow during mechanical insufflation-exsufflation in people with cervical spinal cord injury: a pilot study.Sci Rep. 2023 Oct 2;13(1):16548. doi: 10.1038/s41598-023-43256-x. Sci Rep. 2023. PMID: 37783754 Free PMC article. Clinical Trial.
-
Expiratory flow limitation during mechanical ventilation: real-time detection and physiological subtypes.Crit Care. 2024 May 21;28(1):171. doi: 10.1186/s13054-024-04953-9. Crit Care. 2024. PMID: 38773629 Free PMC article.
-
Role of inspiratory capacity on dyspnea evaluation in COPD with or without emphysematous lesions: a pilot study.Int J Chron Obstruct Pulmon Dis. 2017 Sep 30;12:2823-2830. doi: 10.2147/COPD.S142016. eCollection 2017. Int J Chron Obstruct Pulmon Dis. 2017. PMID: 29033563 Free PMC article.
References
-
- Pride NB, Milic-Emili J. Lung mechanics. In: Calverley P, Pride NB, editors. Chronic Obstructive Lung Disease. London, UK: Chapman Hall; 1995. pp. 135–160.
-
- Fry DL, Hyatt RE. Pulmonary mechanics. A unified analysis of the relationship between pressure, volume and gasflow in the lungs of normal and diseased human subjects. The American Journal of Medicine. 1960;29(4):672–689. - PubMed
-
- Pride NB. Ageing and changes in lung mechanics. European Respiratory Journal. 2005;26(4):563–565. - PubMed
-
- Tucker DH, Sieker HO. The effect of change in body position on lung volumes and intrapulmonary gas mixing in patients with obesity, heart failure, and emphysema. The American Review of Respiratory Disease. 1984;129:101–105. - PubMed
-
- Castile R, Mead J, Jackson A, Wohl ME, Stokes D. Effects of posture on flow-volume curve configuration in normal humans. Journal of Applied Physiology Respiratory Environmental and Exercise Physiology. 1982;53(5):1175–1183. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
