

A study of bone mineral density and its determinants in type 1 diabetes mellitus
- PMID: 23607045
- PMCID: PMC3628496
- DOI: 10.1155/2013/397814
A study of bone mineral density and its determinants in type 1 diabetes mellitus
Abstract
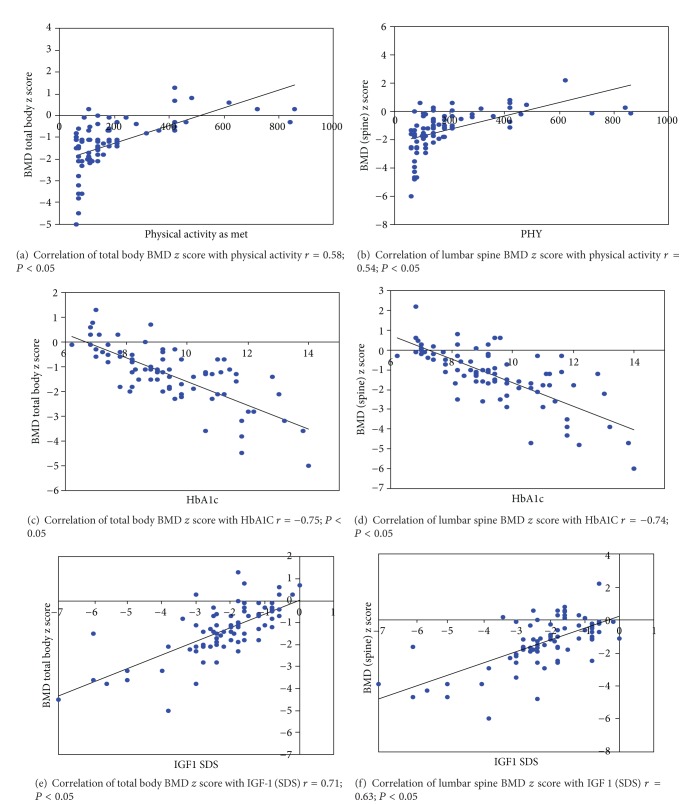
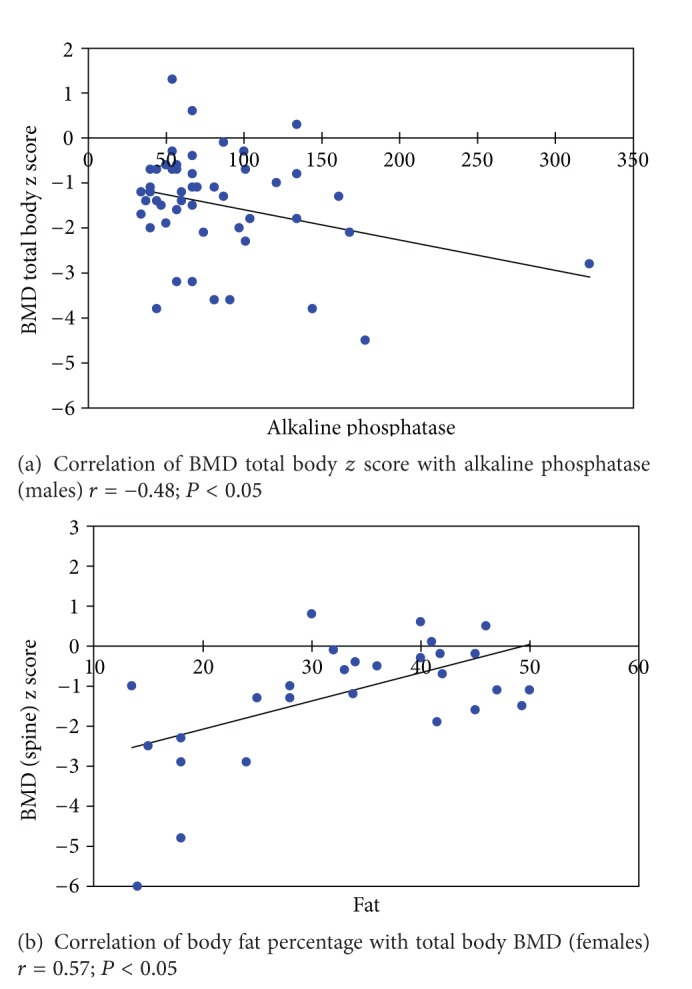
Type 1 diabetes mellitus (T1DM) has been inconsistently associated with low bone mineral density (BMD) and increased fracture risk. 86 consecutive T1DM cases and 140 unrelated age and sex matched healthy nondiabetic controls were included in the study. After history and examination, BMD and body composition were assessed by dual energy X-ray absorptiometry (DXA). Serum samples were analyzed for calcium, phosphorus, albumin, creatinine, alkaline phosphatase, 25 (OH) vitamin D3, intact parathormone (PTH) levels (both cases and controls) and HbA1c, antimicrosomal and IgA tissue transglutaminase (IgA TTG) antibodies, cortisol, follicle stimulating hormone (FSH), testosterone, sex hormone binding globulin (SHBG), tetraiodothyronine (T4), thyroid stimulating hormone (TSH), growth hormone (GH), insulin-like growth factor-1 (IGF-1), and insulin-like growth factor binding protein 3 (IGFBP3) (cases only). T1DM cases had a lower BMD as compared to controls at both total body (TB) and lumbar spine (LS) (P < 0.05). Patients with celiac autoimmunity (CA) had significantly, lower BMD as compared to age, sex, and body mass index (BMI) matched T1DM controls. Linear regression analysis showed that low BMD in T1DM patients was associated with poor glycaemic control, lower IGF-1 levels, less physical activity (in total population as well as in male and female subgroups), and lower body fat percentage (in females) and higher alkaline phosphatase level (in males) (P < 0.05).
Figures
References
-
- Vestergaard P. Discrepancies in bone mineral density and fracture risk in patients with type 1 and type 2 diabetes—a meta-analysis. Osteoporosis International. 2007;18(4):427–444. - PubMed
-
- Janghorbani M, van Dam RM, Willett WC, Hu FB. Systematic review of type 1 and type 2 diabetes mellitus and risk of fracture. American Journal of Epidemiology. 2007;166(5):495–505. - PubMed
-
- Strotmeyer E, Cauler J. Diabetes mellitus, bone mineral density, and fracture risk. Current Opinion in Endocrinology, Diabetes and Obesity. 2007;14(6):429–435. - PubMed
-
- Hagstromer M, Oja P, Sjostrom M. The International Physical Activity Questionnaire (IPAQ): a study of concurrent and construct validity. Public Health Nutrition. 2006;9(6):755–762. - PubMed
-
- Warner JT, Cowan FJ, Dunstan FDJ, Evans WD, Webb DKH, Gregory JW. Measured and predicted bone mineral content in healthy boys and girls aged 6–18 years: adjustment for body size and puberty. Acta Paediatrica. 1998;87(3):244–249. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
