

White coat hypertension is more risky than prehypertension: important role of arterial wave reflections
- PMID: 23608649
- PMCID: PMC4536898
- DOI: 10.1161/HYPERTENSIONAHA.111.00569
White coat hypertension is more risky than prehypertension: important role of arterial wave reflections
Abstract
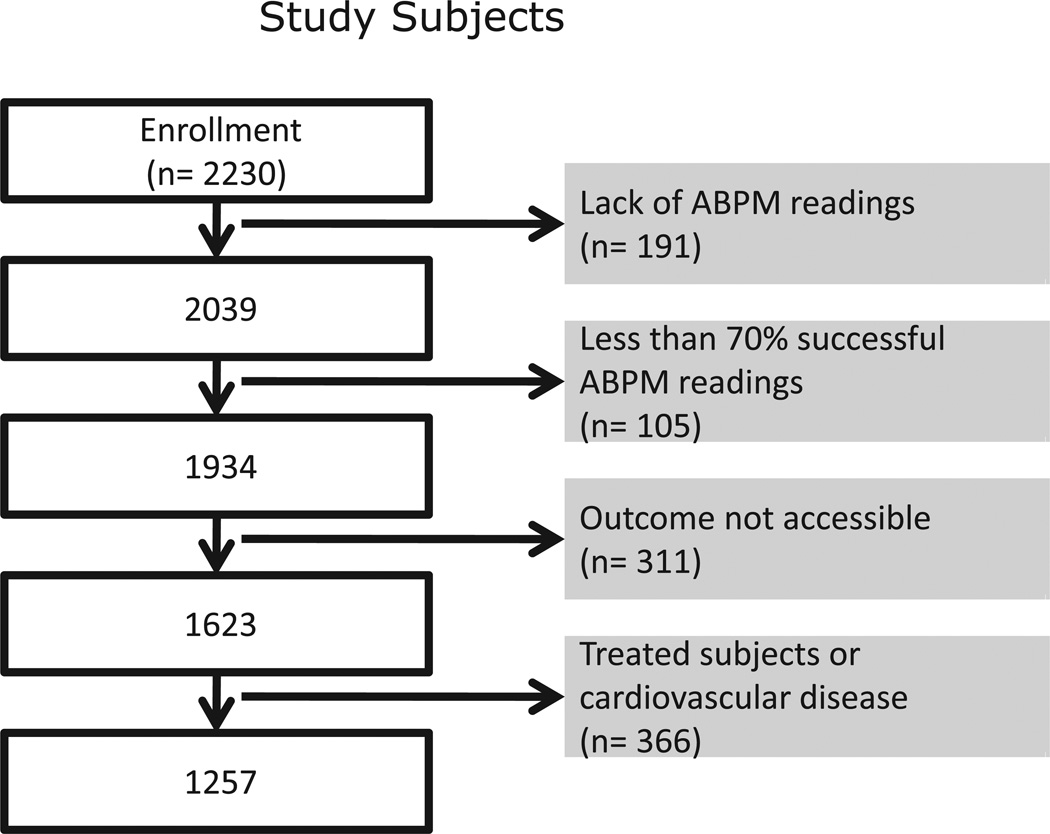
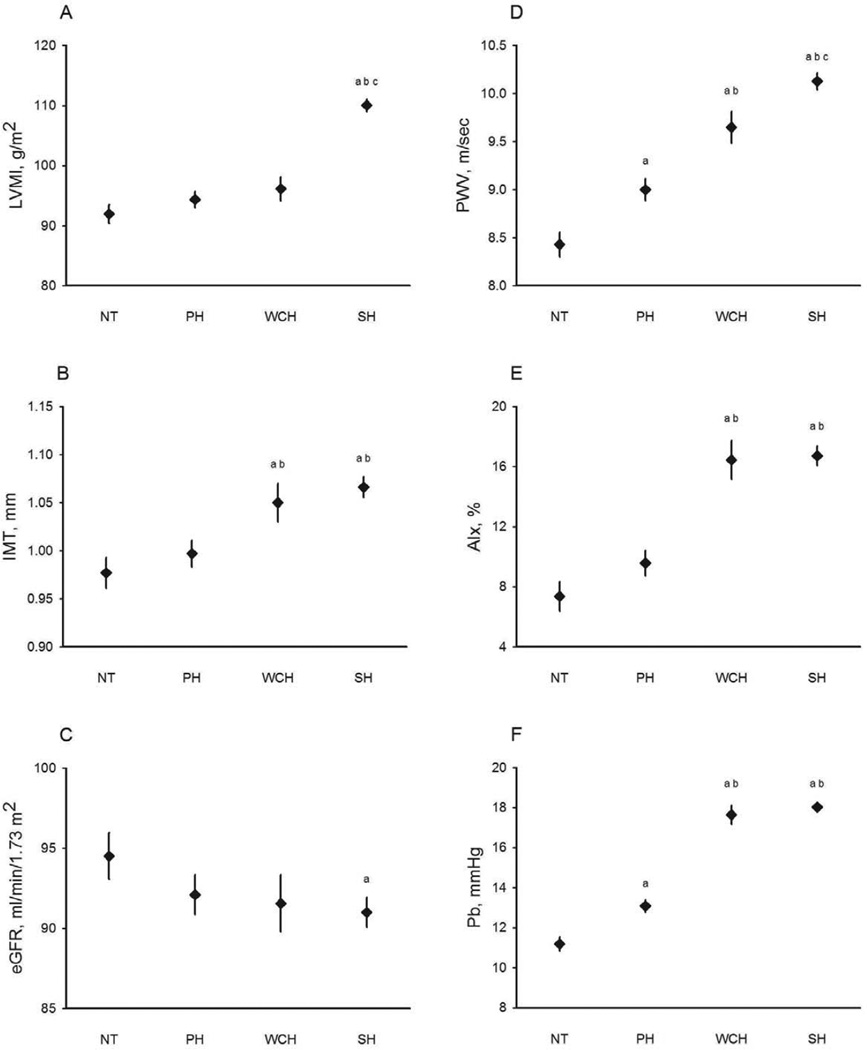
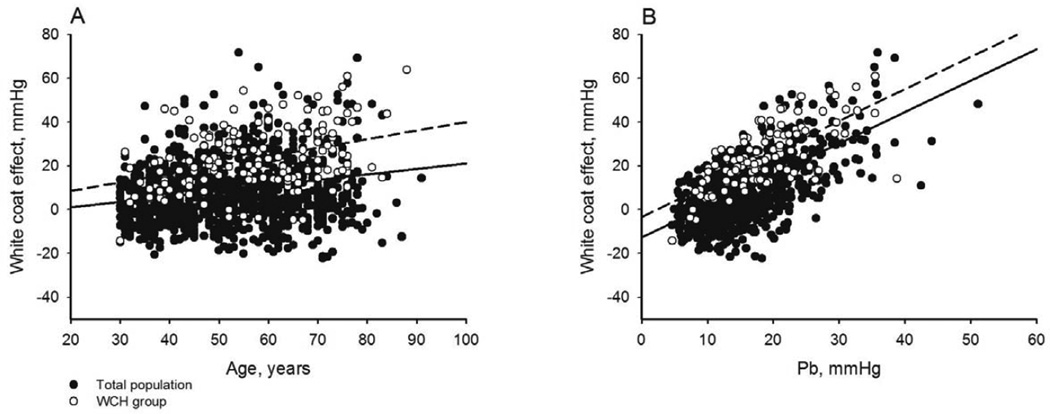
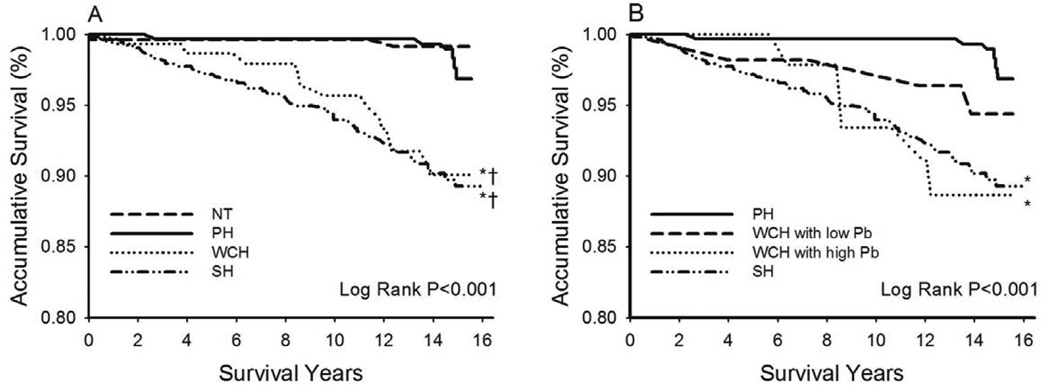
Arterial aging may link cardiovascular risk to white coat hypertension (WCH). The aims of the present study were to investigate the role of arterial aging in the white coat effect, defined as the difference between office and 24-hour ambulatory systolic blood pressures, and to compare WCH with prehypertension (PH) with respect to target organ damage and long-term cardiovascular mortality. A total of 1257 never-been-treated volunteer subjects from a community-based survey were studied. WCH and PH were defined by office and 24-hour ambulatory blood pressures. Left ventricular mass index, carotid intima-media thickness, estimated glomerular filtration rate, carotid-femoral pulse wave velocity, carotid augmentation index, amplitude of the reflection pressure wave, and 15-year cardiovascular mortality were determined. Subjects with WCH were significantly older and had greater body mass index, blood pressure values, intima-media thickness, carotid-femoral pulse wave velocity, augmentation index, amplitude of the backward pressure wave, and a lower estimated glomerular filtration rate than PH. Amplitude of the backward pressure wave was the most important independent correlate of the white coat effect in multivariate analysis (model r(2)=0.451; partial r(2)/model r(2)=90.5%). WCH had significantly greater cardiovascular mortality than PH (hazard ratio, 2.94; 95% confidence interval, 1.09-7.91), after accounting for age, sex, body mass index, smoking, fasting plasma glucose, and total cholesterol/high-density lipoprotein-cholesterol ratio. Further adjustment of the model for amplitude of the backward pressure wave eliminated the statistical significance of the WCH effect. In conclusion, the white coat effect is mainly caused by arterial aging. WCH carries higher risk for cardiovascular mortality than PH, probably via enhanced wave reflections that accompany arterial aging.
Keywords: arterial aging; arterial wave reflections; cardiovascular mortality; prehypertension; white coat hypertension.
Conflict of interest statement
None
Figures
References
-
- Guo F, He D, Zhang W, Walton RG. Trends in prevalence, awareness, management, and control of hypertension among united states adults, 1999 to 2010. J Am Coll Cardiol. 2012;60:599–606. - PubMed
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, Jones DW, Materson BJ, Oparil S, Wright JT, Jr, Roccella EJ. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: The jnc 7 report. JAMA. 2003;289:2560–2572. - PubMed
-
- Vasan RS, Larson MG, Leip EP, Evans JC, O’Donnell CJ, Kannel WB, Levy D. Impact of high-normal blood pressure on the risk of cardiovascular disease. N Engl J Med. 2001;345:1291–1297. - PubMed
-
- Qureshi AI, Suri MF, Kirmani JF, Divani AA, Mohammad Y. Is prehypertension a risk factor for cardiovascular diseases? Stroke. 2005;36:1859–1863. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
