

Disparities in trauma care and outcomes in the United States: a systematic review and meta-analysis
- PMID: 23609267
- PMCID: PMC3641534
- DOI: 10.1097/TA.0b013e31828c331d
Disparities in trauma care and outcomes in the United States: a systematic review and meta-analysis
Abstract
Background: Race and socioeconomic disparities are pervasive and persist throughout our health care system. Inequities have also been identified in outcomes after trauma despite its immediate nature and the perceived equal access to emergent care.
Objectives: Our objective was to systematically evaluate the current literature on the association between trauma mortality and race, insurance status, and socioeconomic status. Our secondary objective was to assess data investigating potential mechanisms underlying these outcome disparities.
Methods: We performed a systematic review and random effects meta-analysis to examine the relationship between trauma and race, insurance, and socioeconomic disparities published between April 1990 and October 2011. The Cochrane Review Handbook and the Meta-Analysis of Observational Studies in Epidemiology (MOOSE) statement were used as guides.
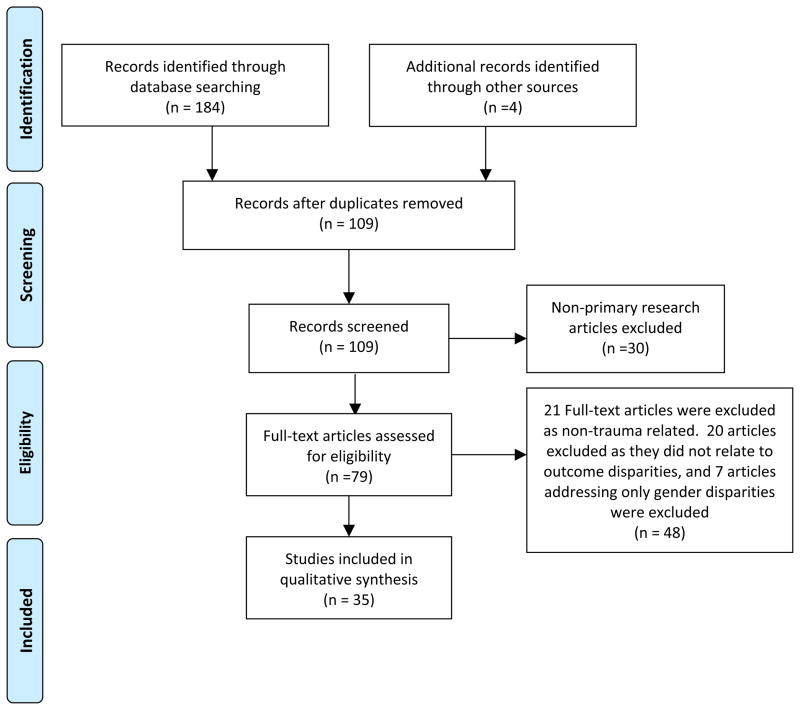
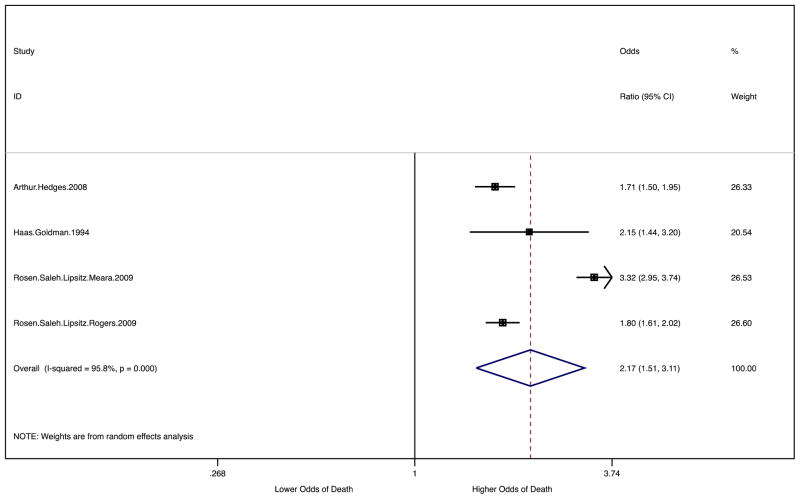
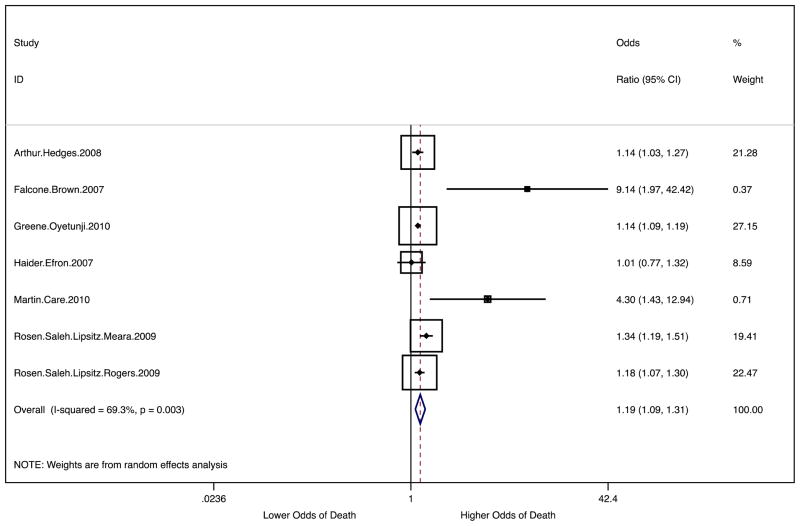
Results: Thirty-five studies were included in the final review. The current body of literature indicates that uninsured status is an independent negative predictor of trauma outcomes. Our meta-analysis corroborated this by demonstrating that uninsured patients were more likely to die than privately insured patients (OR 2.17 95% CI 1.51–3.11). Racial disparities in trauma outcomes are shown to be present and independent for black patients compared to whites. Our meta-analysis demonstrated that black race was associated with higher odds of death when compared with white race (OR 1.19 95% CI 1.09 – 1.31). Studies comparing Hispanic and white non-Hispanic patients’ post-trauma mortality outcomes, however, have provided conflicting results. Our meta-analysis found no significant difference in mortality comparing Hispanic patients with white patients (OR 1.08 95% CI 0.99–1.18)
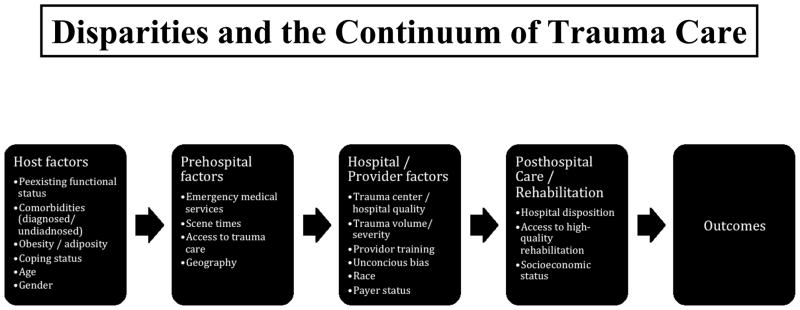
Conclusions: Both race/ethnicity and insurance are clearly associated with disparate outcomes following trauma. These disparities are likely due to myriad factors across the trauma continuum of care: host factors, prehospital factors, hospital/provider factors, and factors associated with postacute care and rehabilitation. While there are many proposed mechanisms, we believe that there are several interventions that could be particularly effective in combatting trauma disparities. These include trauma prevention programs targeting vulnerable populations, expansion of healthcare coverage, relocation of trauma centers to better provide for vulnerable populations, and restructuring clinical training to address implicit biases. While much work still remains to fully elucidate the mechanisms underlying trauma disparities, we can and should now act to begin to reduce or eliminate these disparities that still plague our healthcare system.
Level of Evidence: Two.
Conflict of interest statement
None.
Figures
References
-
- Kochanek KD, Xu J, Murphy SL, Minino AM, Kung HC. Deaths: final data for 2009. National vital statistics reports: from the Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System. 2011;60(3):1–166. - PubMed
-
- Arango-Lasprilla JC, Rosenthal M, Deluca J, Cifu DX, Hanks R, Komaroff E. Functional outcomes from inpatient rehabilitation after traumatic brain injury: how do Hispanics fare? Archives of physical medicine and rehabilitation. 2007 Jan;88(1):11–18. - PubMed
-
- Arango-Lasprilla JC, Rosenthal M, Deluca J, et al. Traumatic brain injury and functional outcomes: does minority status matter? Brain injury: [BI] 2007 Jun;21(7):701–708. - PubMed
-
- Nirula R, Nirula G, Gentilello LM. Inequity of rehabilitation services after traumatic injury. The Journal of trauma. 2009 Jan;66(1):255–259. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
