

The trade-offs in field trauma triage: a multiregion assessment of accuracy metrics and volume shifts associated with different triage strategies
- PMID: 23609282
- PMCID: PMC3726266
- DOI: 10.1097/TA.0b013e31828b7848
The trade-offs in field trauma triage: a multiregion assessment of accuracy metrics and volume shifts associated with different triage strategies
Abstract
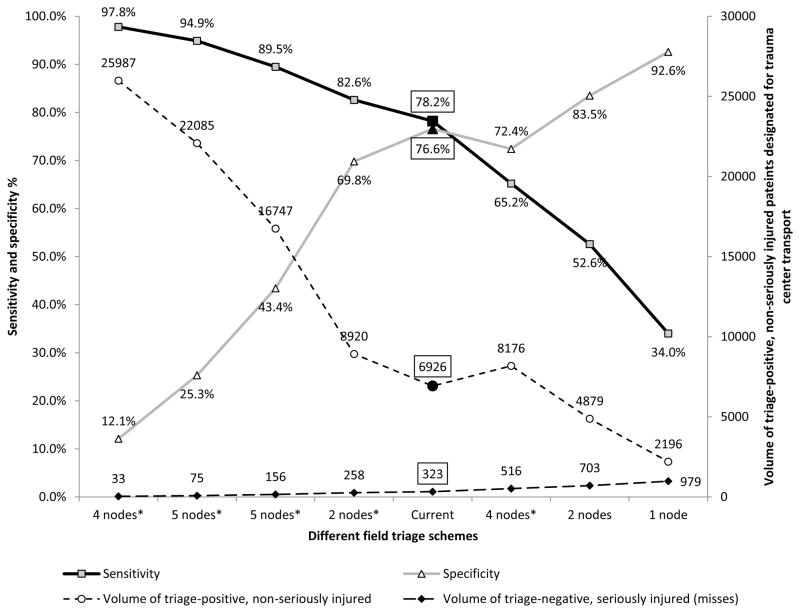
Background: National benchmarks for trauma triage sensitivity (≥95%) and specificity (≥50%) have not been rigorously evaluated across broad populations of injured patients. We evaluated the impact of different field triage schemes for identifying seriously injured patients across a range of sensitivity values. Impact metrics included specificity and number of undertriaged and overtriaged patients compared with current triage practices.
Methods: This was a retrospective cohort study of injured children and adults transported by 48 emergency medical service (EMS) agencies to 105 hospitals in 6 regions of the Western United States from 2006 through 2008. Hospital outcomes were probabilistically linked to EMS records through trauma registries, state discharge databases, and state emergency department databases. The primary outcome was an Injury Severity Score (ISS) of 16 or greater. We evaluated 40 field predictor variables, including 31 current field triage criteria, using classification and regression tree analysis and cross-validation to generate estimates for sensitivity and specificity.
Results: A total of 89,261 injured patients were evaluated and transported by EMS providers during the 3-year period, of whom 5,711 (6.4%) had ISS of 16 or greater. As the 95% sensitivity target for triage was approached (from the current value of 87.5%), decision tree complexity increased, specificity decreased (from 62.8% to 18.7%), and the number of triage-positive patients without serious injury doubled (67,927 vs. 31,104). Analyses restricted to children and older adults were similar. The most consistent modification to the current triage algorithm to increase sensitivity without a major decrease in specificity was altering the Glasgow Coma Scale (GCS) score cutoff point from 13 or less to 14 or less (sensitivity increase to 90.4%).
Conclusion: Reaching the field triage sensitivity benchmark of 95% would require a large decrease in specificity (increase in overtriage). A 90% sensitivity target seems more realistic and may be obtainable by modest changes to the current triage algorithm.
Conflict of interest statement
There are no conflicts of interest among authors for this paper.
Figures



References
-
- Mackersie RC. History of Trauma Field Triage Development and the American College of Surgeons Criteria. Prehospital Emerg Care. 2006;10(3):287–294. - PubMed
-
- Bulletin of the American College of Surgeons. Sep, 1976.
-
- Hospital and Prehospital Resources for the Optimal Care of the Injured Patient. Chicago, IL: American College of Surgeons; 1987.
-
- Field categorization of trauma patients. Bull Am Coll Surg. 1986;71:17–21.
-
- Resources for the Optimal Care of the Injured Patient. Chicago, IL: Amer College of Surgeons; 1990.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
