

Preeclampsia as a risk factor for diabetes: a population-based cohort study
- PMID: 23610560
- PMCID: PMC3627640
- DOI: 10.1371/journal.pmed.1001425
Preeclampsia as a risk factor for diabetes: a population-based cohort study
Abstract
Background: Women with preeclampsia (PEC) and gestational hypertension (GH) exhibit insulin resistance during pregnancy, independent of obesity and glucose intolerance. Our aim was to determine whether women with PEC or GH during pregnancy have an increased risk of developing diabetes after pregnancy, and whether the presence of PEC/GH in addition to gestational diabetes (GDM) increases the risk of future (postpartum) diabetes.
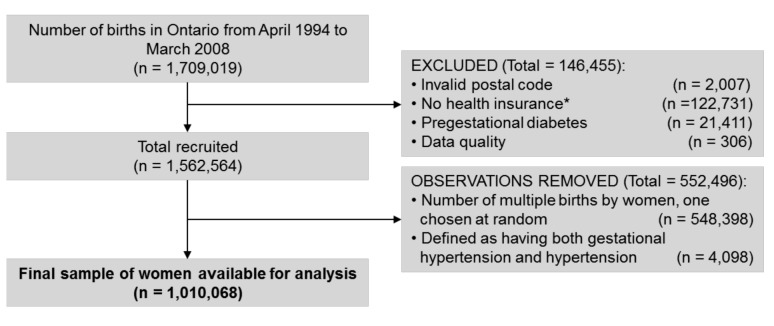
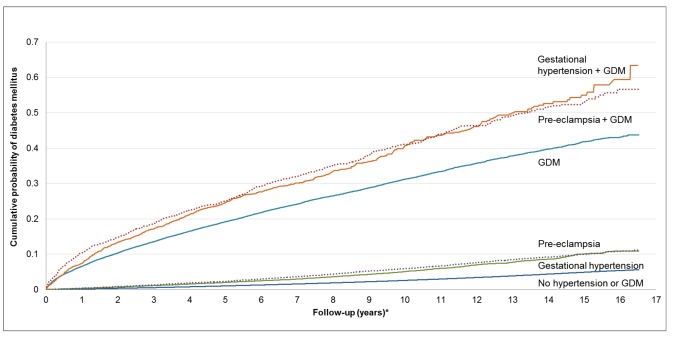
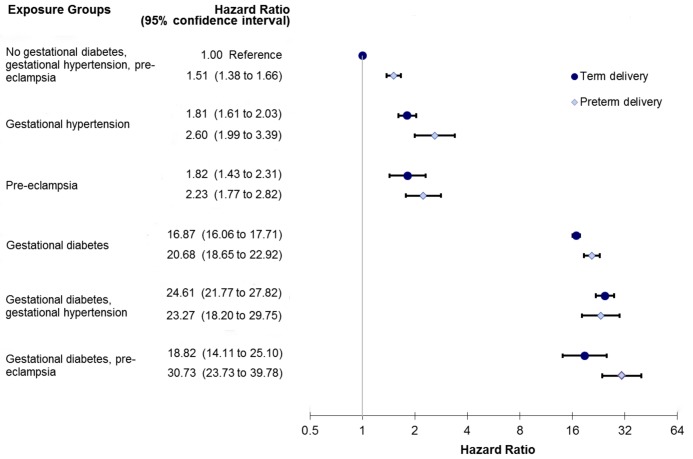
Methods and findings: We performed a population-based, retrospective cohort study for 1,010,068 pregnant women who delivered in Ontario, Canada between April 1994 and March 2008. Women were categorized as having PEC alone (n=22,933), GH alone (n=27,605), GDM alone (n=30,852), GDM+PEC (n=1,476), GDM+GH (n=2,100), or none of these conditions (n=925,102). Our main outcome was a new diagnosis of diabetes postpartum in the following years, up until March 2011, based on new records in the Ontario Diabetes Database. The incidence rate of diabetes per 1,000 person-years was 6.47 for women with PEC and 5.26 for GH compared with 2.81 in women with neither of these conditions. In the multivariable analysis, both PEC alone (hazard ratio [HR]=2.08; 95% CI 1.97-2.19) and GH alone (HR=1.95; 95% CI 1.83-2.07) were risk factors for subsequent diabetes. Women with GDM alone were at elevated risk of developing diabetes postpartum (HR=12.77; 95% CI 12.44-13.10); however, the co-presence of PEC or GH in addition to GDM further elevated this risk (HR=15.75; 95% CI 14.52-17.07, and HR=18.49; 95% CI 17.12-19.96, respectively). Data on obesity were not available.
Conclusions: Women with PEC/GH have a 2-fold increased risk of developing diabetes when followed up to 16.5 years after pregnancy, even in the absence of GDM. The presence of PEC/GH in the setting of GDM also raised the risk of diabetes significantly beyond that seen with GDM alone. A history of PEC/GH during pregnancy should alert clinicians to the need for preventative counseling and more vigilant screening for diabetes. Please see later in the article for the Editors' Summary.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Comment in
-
Is it time to screen women with history of hypertensive pregnancy disorders for diabetes?PLoS Med. 2013;10(4):e1001428. doi: 10.1371/journal.pmed.1001428. Epub 2013 Apr 16. PLoS Med. 2013. PMID: 23610563 Free PMC article.
-
Diabetes: Pre-eclampsia: association with increased risk of diabetes.Nat Rev Nephrol. 2013 Jul;9(7):372. doi: 10.1038/nrneph.2013.96. Epub 2013 May 7. Nat Rev Nephrol. 2013. PMID: 23649017 No abstract available.
Similar articles
-
Considering parents as a unit: Associations of gestational diabetes and gestational hypertension with postpartum diabetes and hypertension in couples.Pregnancy Hypertens. 2019 Apr;16:32-37. doi: 10.1016/j.preghy.2019.02.004. Epub 2019 Feb 18. Pregnancy Hypertens. 2019. PMID: 31056157
-
Polycystic ovary syndrome as an independent risk factor for gestational diabetes and hypertensive disorders of pregnancy: a population-based study on 9.1 million pregnancies.Hum Reprod. 2020 Jul 1;35(7):1666-1674. doi: 10.1093/humrep/deaa099. Hum Reprod. 2020. PMID: 32535629
-
Conjoint Associations of Gestational Diabetes and Hypertension With Diabetes, Hypertension, and Cardiovascular Disease in Parents: A Retrospective Cohort Study.Am J Epidemiol. 2017 Nov 15;186(10):1115-1124. doi: 10.1093/aje/kwx263. Am J Epidemiol. 2017. PMID: 29149255 Free PMC article.
-
Gestational diabetes, pregnancy hypertension, and late vascular disease.Diabetes Care. 2007 Jul;30 Suppl 2:S246-50. doi: 10.2337/dc07-s224. Diabetes Care. 2007. PMID: 17596480 Review.
-
Epidemiology of gestational diabetes mellitus and its association with Type 2 diabetes.Diabet Med. 2004 Feb;21(2):103-13. doi: 10.1046/j.1464-5491.2003.00985.x. Diabet Med. 2004. PMID: 14984444 Review.
Cited by
-
Diabetes after pregnancy: a study protocol for the derivation and validation of a risk prediction model for 5-year risk of diabetes following pregnancy.Diagn Progn Res. 2021 Mar 8;5(1):5. doi: 10.1186/s41512-021-00095-6. Diagn Progn Res. 2021. PMID: 33678196 Free PMC article.
-
Circulating levels of angiogenic factors and their association with preeclampsia among pregnant women at Mulago National Referral Hospital in Uganda.PLoS One. 2021 May 19;16(5):e0251227. doi: 10.1371/journal.pone.0251227. eCollection 2021. PLoS One. 2021. PMID: 34010327 Free PMC article.
-
Estimating rate of insulin resistance in patients with preeclampsia using HOMA-IR index and comparison with nonpreeclampsia pregnant women.Biomed Res Int. 2014;2014:140851. doi: 10.1155/2014/140851. Epub 2014 Apr 9. Biomed Res Int. 2014. PMID: 24812607 Free PMC article.
-
Is it time to screen women with history of hypertensive pregnancy disorders for diabetes?PLoS Med. 2013;10(4):e1001428. doi: 10.1371/journal.pmed.1001428. Epub 2013 Apr 16. PLoS Med. 2013. PMID: 23610563 Free PMC article.
-
Preeclampsia and Neurodevelopmental Outcomes: Potential Pathogenic Roles for Inflammation and Oxidative Stress?Mol Neurobiol. 2021 Jun;58(6):2734-2756. doi: 10.1007/s12035-021-02290-4. Epub 2021 Jan 25. Mol Neurobiol. 2021. PMID: 33492643 Review.
References
-
- Zimmet PZ, Alberti KGMM (2006) Introduction: globalization and the non–communicable disease epidemic. Obesity 14: 1–3. - PubMed
-
- Lipscombe LL, Hux JE (2007) Trends in diabetes prevalence, incidence, and mortality in Ontario, Canada 1995–2005: a population-based study. Lancet 369: 750–756. - PubMed
-
- Diabetes Prevention Program Research Group (2002) N Eng J Med 346: 393–403. - PubMed
-
- Tuomilehto J, Lindström J, Eriksson JG, Valle TT, Hämäläinen H, et al. (2001) Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Eng J Med 344: 1343–1350. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
