

Pathological fractures in children
- PMID: 23610658
- PMCID: PMC3626256
- DOI: 10.1302/2046-3758.110.2000120
Pathological fractures in children
Abstract
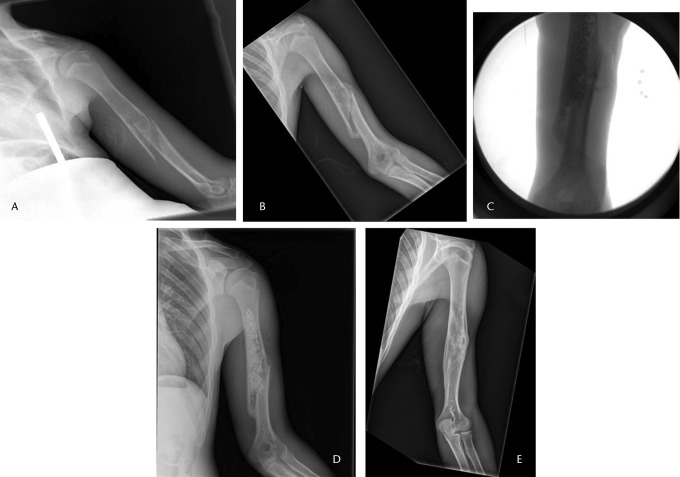
Pathological fractures in children can occur as a result of a variety of conditions, ranging from metabolic diseases and infection to tumours. Fractures through benign and malignant bone tumours should be recognised and managed appropriately by the treating orthopaedic surgeon. The most common benign bone tumours that cause pathological fractures in children are unicameral bone cysts, aneurysmal bone cysts, non-ossifying fibromas and fibrous dysplasia. Although pathological fractures through a primary bone malignancy are rare, these should be recognised quickly in order to achieve better outcomes. A thorough history, physical examination and review of plain radiographs are crucial to determine the cause and guide treatment. In most benign cases the fracture will heal and the lesion can be addressed at the time of the fracture, or after the fracture is healed. A step-wise and multidisciplinary approach is necessary in caring for paediatric patients with malignancies. Pathological fractures do not have to be treated by amputation; these fractures can heal and limb salvage can be performed when indicated.
Keywords: Benign; Bone tumour; Children; Malignancy; Pathological fracture; Sarcoma.
Conflict of interest statement
Figures


References
-
- Dormans JP, Pill SG. Fractures through bone cysts: unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457–467 - PubMed
-
- Snyder BD, Hauser-Kara DA, Hipp JA, et al. Predicting fracture through benign skeletal lesions with quantitative computed tomography. J Bone Joint Surg [Am] 2006;88-A:55–70 - PubMed
-
- Easley ME, Kneisl JS. Pathologic fractures through nonossifying fibromas: is prophylactic treatment warranted? J Pediatr Orthop 1997;17:808–813 - PubMed
-
- Kaelin AJ, MacEwen GD. Unicameral bone cysts: natural history and the risk of fracture. Int Orthop 1989;13:275–282 - PubMed
