

Boosted selective internal radiation therapy with 90Y-loaded glass microspheres (B-SIRT) for hepatocellular carcinoma patients: a new personalized promising concept
- PMID: 23613103
- PMCID: PMC3679421
- DOI: 10.1007/s00259-013-2395-x
Boosted selective internal radiation therapy with 90Y-loaded glass microspheres (B-SIRT) for hepatocellular carcinoma patients: a new personalized promising concept
Abstract
Purpose: To evaluate the impact of dosimetry based on MAA SPECT/CT for the prediction of response, toxicity and survival, and for treatment planning in patients with hepatocellular carcinoma (HCC) treated with (90)Y-loaded glass microspheres (TheraSphere®).
Methods: TheraSphere® was administered to 71 patients with inoperable HCC. MAA SPECT/CT quantitative analysis was used for the calculation of the tumour dose (TD), healthy injected liver dose (HILD), and total injected liver dose. Response was evaluated at 3 months using EASL criteria. Time to progression (TTP) and overall survival (OS) were evaluated using the Kaplan-Meier method. Factors potentially associated with liver toxicity were combined to construct a liver toxicity score (LTS).
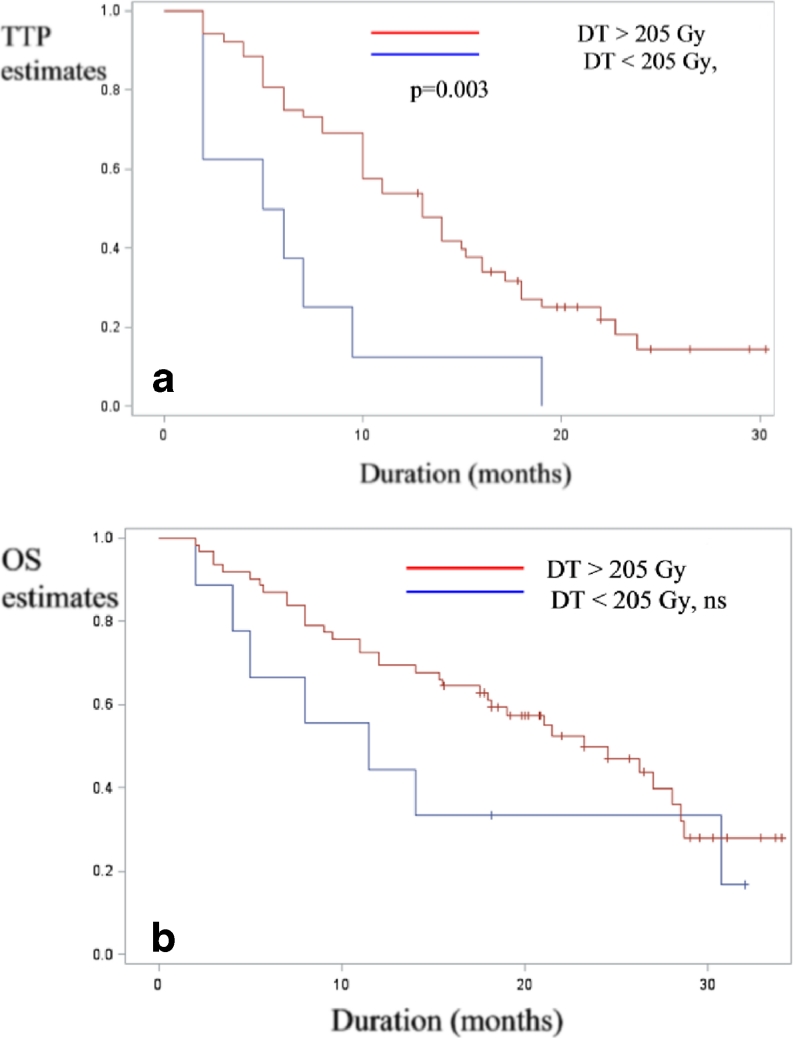
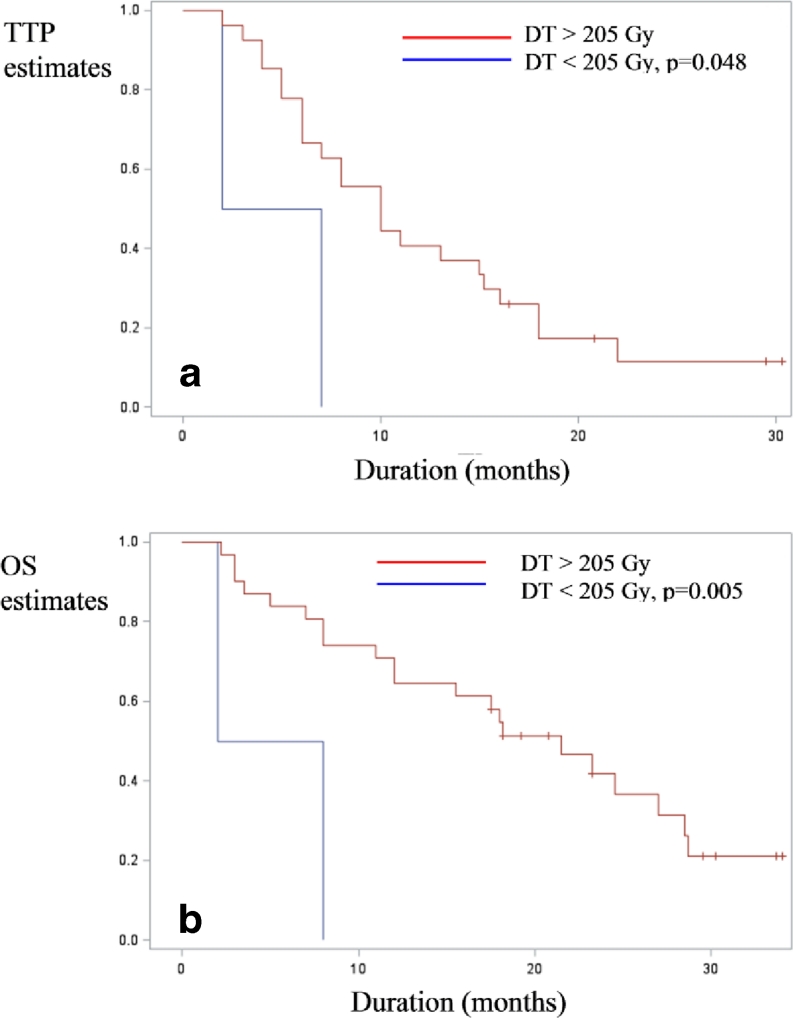
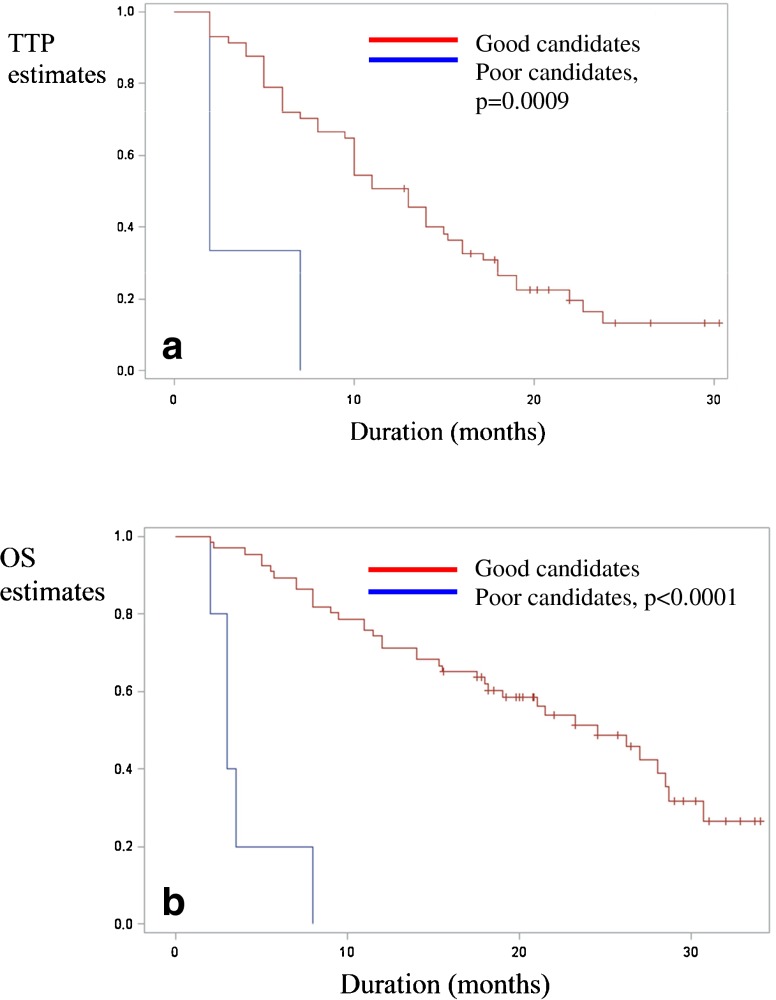
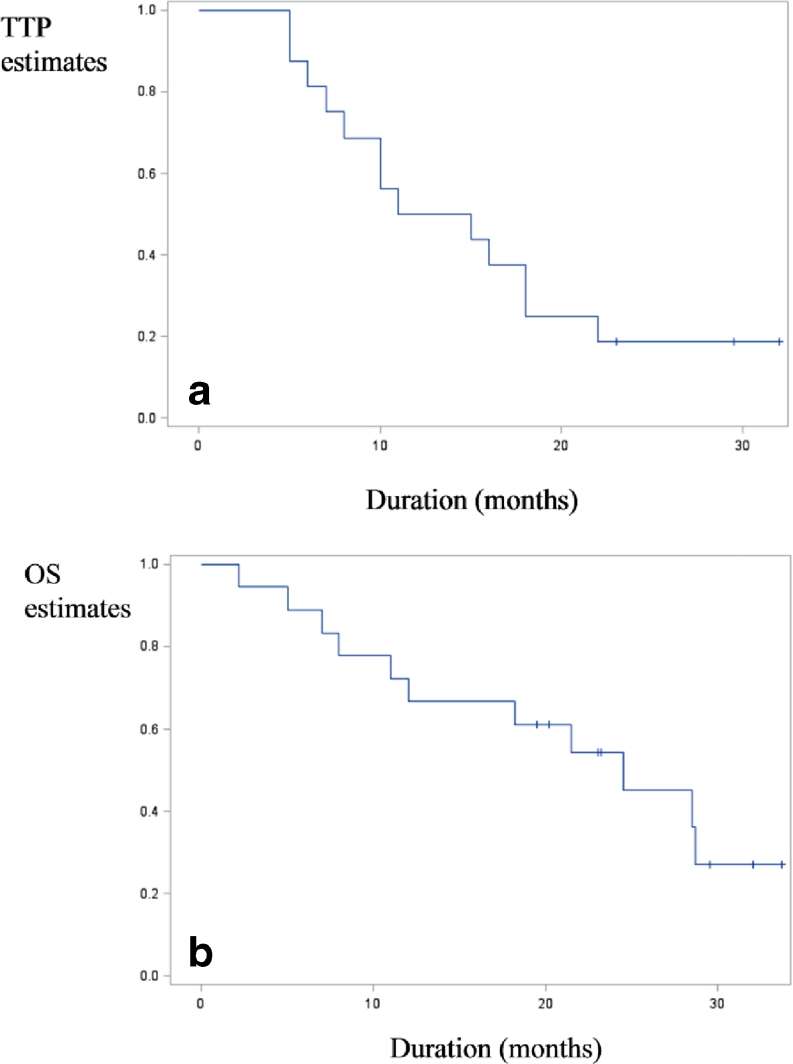
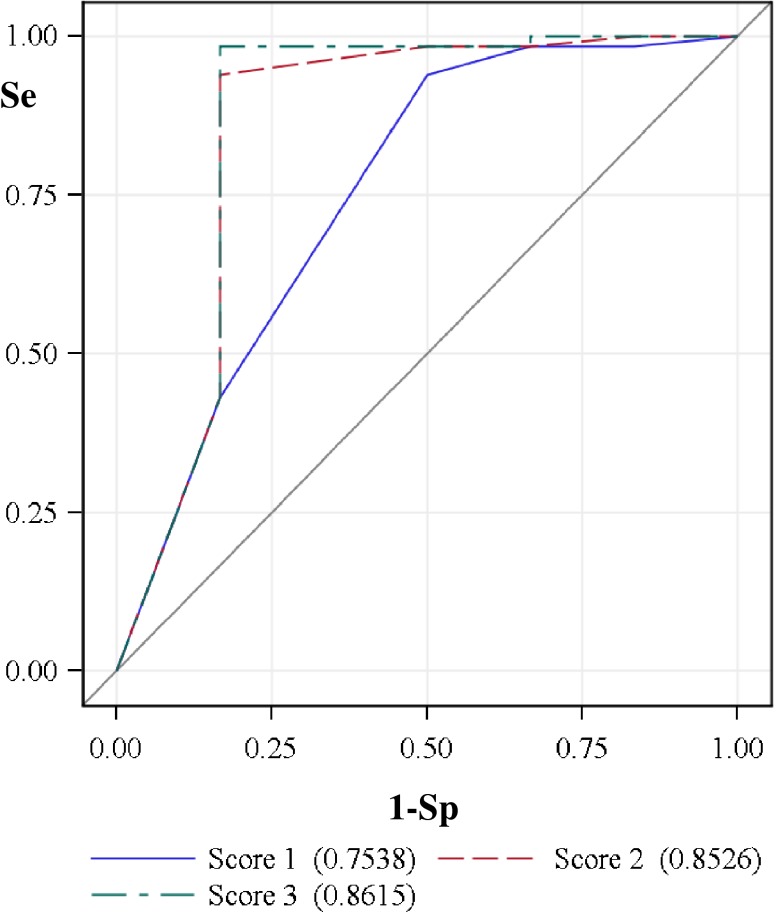
Results: The response rate was 78.8%. Median TD were 342 Gy for responding lesions and 191 Gy for nonresponding lesions (p < 0.001). With a threshold TD of 205 Gy, MAA SPECT/CT predicted response with a sensitivity of 100% and overall accuracy of 90%. Based on TD and HILD, 17 patients underwent treatment intensification resulting in a good response rate (76.4%), without increased grade III liver toxicity. The median TTP and OS were 5.5 months (2-9.5 months) and 11.5 months (2-31 months), respectively, in patients with TD <205 Gy and 13 months (10-16 months) and 23.2 months (17.5-28.5 months), respectively, in those with TD >205 Gy (p = 0.0015 and not significant). Among patients with portal vein thrombosis (PVT) (n = 33), the median TTP and OS were 4.5 months (2-7 months) and 5 months (2-8 months), respectively, in patients with TD <205 Gy and 10 months (6-15.2 months) and 21.5 months (12-28.5 months), respectively, in those with TD >205 Gy (p = 0.039 and 0.005). The median OS was 24.5 months (18-28.5 months) in PVT patients with TD >205 Gy and good PVT targeting on MAA SPECT/CT. The LTS was able to detect severe liver toxicity (n = 6) with a sensitivity of 83% and overall accuracy of 97%.
Conclusion: Dosimetry based on MAA SPECT/CT was able to accurately predict response and survival in patients treated with glass microspheres. This method can be used to adapt the injected activity without increasing liver toxicity, thus defining a new concept of boosted selective internal radiation therapy (B-SIRT). This new concept and LTS enable fully personalized treatment planning with glass microspheres to be achieved.
Figures
References
-
- Raoul JL, Guyader D, Bretagne JF, Duvauferrier R, Bourguet P, Bekhechi D, et al. Randomized controlled trial for hepatocellular carcinoma with portal vein thrombosis: intra-arterial iodine-131-iodized oil versus medical support. J Nucl Med. 1994;35:1782–1787. - PubMed
-
- Mazzaferro V, Sposito C, Bhoori S, Romito R, Chiesa C, Morosi C, et al. Yttrium(90) radioembolization for intermediate-advanced hepatocarcinoma: A phase II study. Hepatology. 2012. doi:10.1002/hep.26014. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
