

Mid-term outcomes following endovascular re-intervention for iliac artery in-stent restenosis
- PMID: 23613343
- PMCID: PMC3836870
- DOI: 10.1002/ccd.24975
Mid-term outcomes following endovascular re-intervention for iliac artery in-stent restenosis
Abstract
Objectives: We sought to evaluate the procedural characteristics and clinical outcomes of endovascular repair for iliac artery (IA) in-stent restenosis (ISR).
Background: An increasing percentage of patients with complex IA occlusive disease are treated with an endovascular approach, but the outcomes of IA-ISR have not been well described.
Methods: We analyzed all endovascular procedures for treatment of IA-ISR performed at our institution between July 2006-December 2010. The primary outcome was primary patency, defined as <50% stenosis as assessed by clinical examination and duplex ultrasonography (DUS).
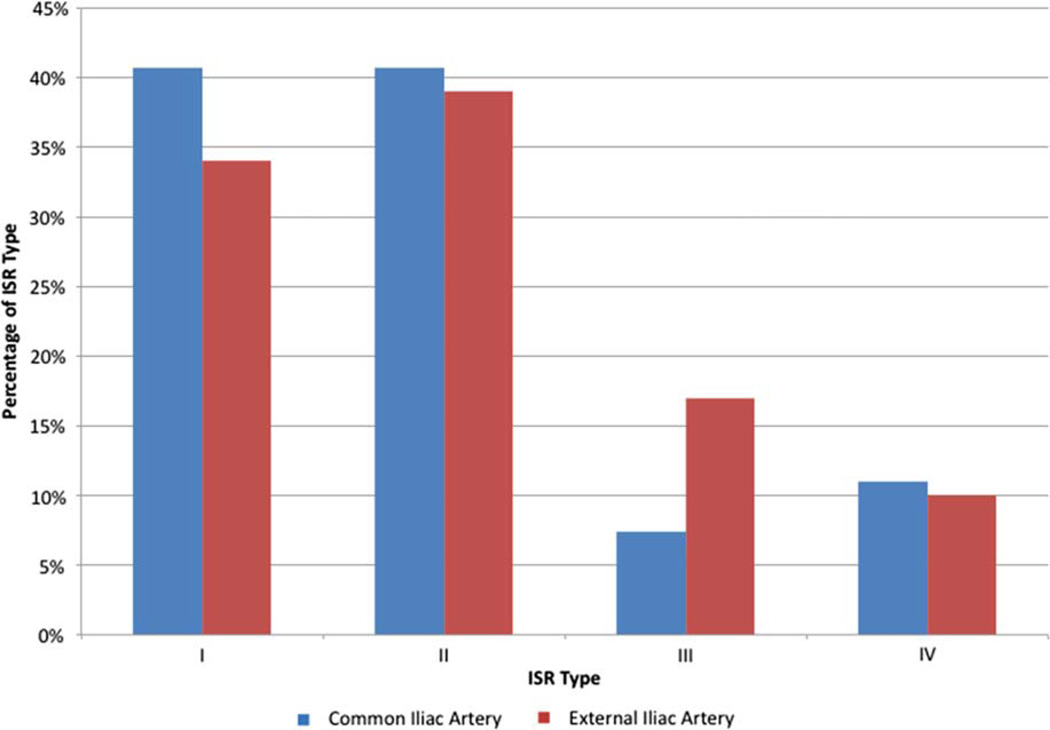
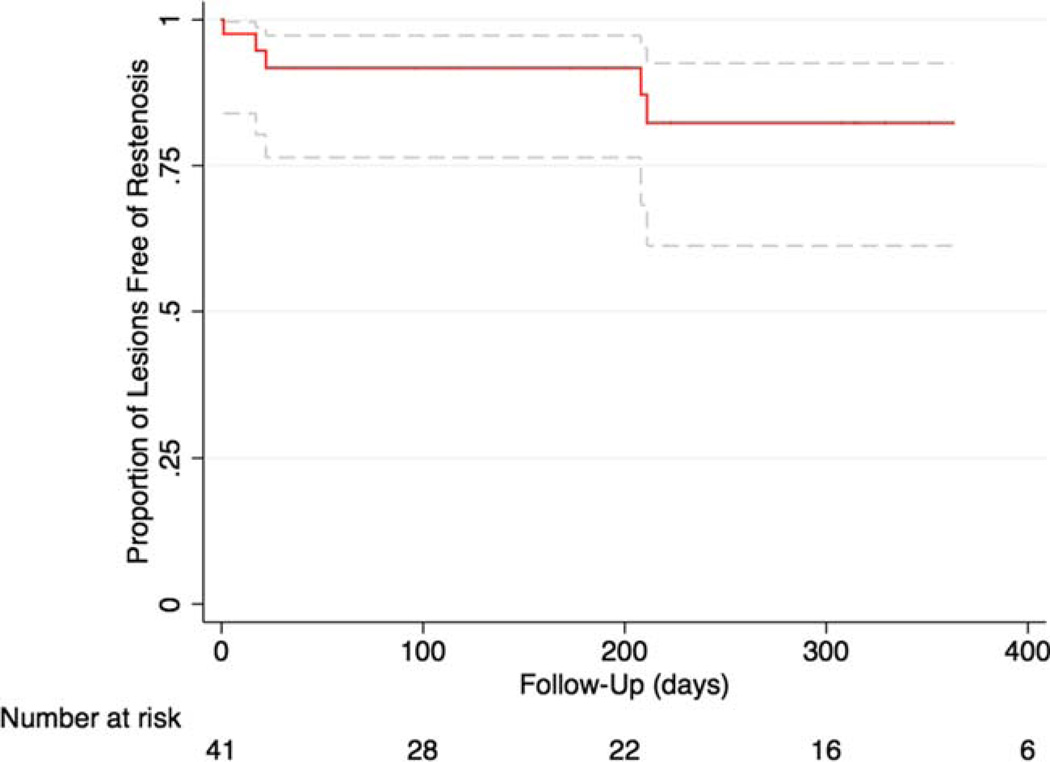
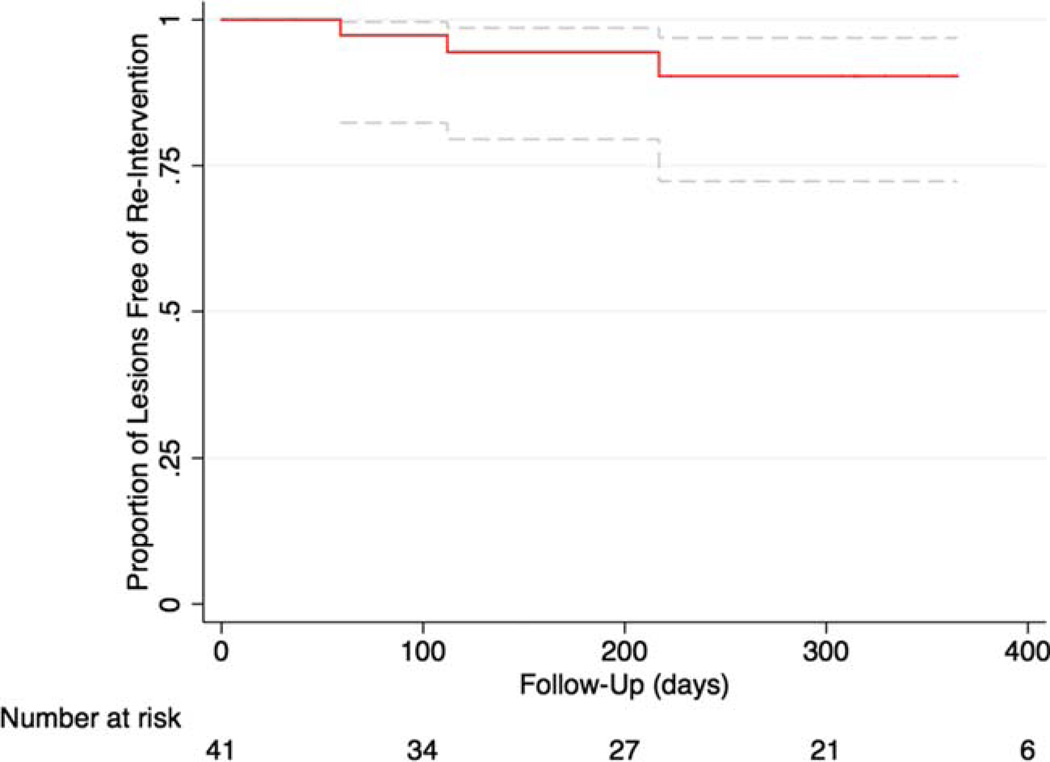
Results: Forty-one lesions in 24 patients who underwent repeated endovascular intervention for treatment of IA-ISR. Most lesions were unilateral and involved the common IA (66%). The mean length of ISR was 30.1 ± 14.1 mm with type I (focal) and II (diffuse) ISR occurring with the greatest frequency (34% and 39%, respectively). All patients underwent balloon angioplasty; adjunctive stenting zwas performed in 27 (66%) of the lesions. Type II ISR lesions more frequently required stenting (13/16 lesions, P = 0.02 compared with other patterns of ISR). Procedural success was 100% with a mean gain of 0.13 in the ankle-brachial index (P = 0.001). The 6- and 12-month primary patency rates were 96% and 82%, respectively. The 12-month primary-assisted patency rate was 90% with clinically driven target lesion revascularization (TLR) in three patients.
Conclusions: Endovascular treatment of IA-ISR using an approach of balloon angioplasty followed by selective stenting is associated with high-patency rates and low rates of TLR at 1 year.
Keywords: iliac artery; in-stent restenosis; peripheral arterial disease.
Copyright © 2013 Wiley Periodicals, Inc.
Conflict of interest statement
Conflict of interest: Nothing to report.
Figures

Comment in
-
Remember those midterms.Catheter Cardiovasc Interv. 2013 Dec 1;82(7):1185-6. doi: 10.1002/ccd.25242. Catheter Cardiovasc Interv. 2013. PMID: 24255034 No abstract available.
References
-
- Vorwerk D, Guenther RW, Schurmann K, Wendt G, Peters I. Primary stent placement for chronic iliac artery occlusions: Follow-up results in 103 patients. Radiology. 1995;194:745–749. - PubMed
-
- Tetteroo E, van der Graaf Y, Bosch JL, van Engelen AD, Hunink MG, Eikelboom BC, et al. Randomised comparison of primary stent placement versus primary angioplasty followed by selective stent placement in patients with iliac-artery occlusive disease. Dutch Iliac Stent Trial Study Group. Lancet. 1998;351(9110):1153–1159. - PubMed
-
- Rees CR, Palmaz JC, Garcia O, Roeren T, Richter GM, Gardiner G, Jr, et al. Angioplasty and stenting of completely occluded iliac arteries. Radiology. 1989;172:953–959. - PubMed
-
- Dyet JF, Gaines PA, Nicholson AA, Cleveland T, Cook AM, Wilkinson AR, et al. Treatment of chronic iliac artery occlusions by means of percutaneous endovascular stent placement. J Vasc Interv Radiol. 1997;8(3):349–353. - PubMed
-
- Yedlicka JW, Jr, Ferral H, Bjarnason H, Hunter DW, Castaneda-Zuniga WR, Amplatz K. Chronic iliac artery occlusions: Primary recanalization with endovascular stents. J Vasc Interv Radiol. 1994;5(6):843–847. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
