

Which patients with chronic obstructive pulmonary disease benefit from the addition of an inhaled corticosteroid to their bronchodilator? A cluster analysis
- PMID: 23613569
- PMCID: PMC3641457
- DOI: 10.1136/bmjopen-2012-001838
Which patients with chronic obstructive pulmonary disease benefit from the addition of an inhaled corticosteroid to their bronchodilator? A cluster analysis
Abstract
Objective: To identify subsets of chronic obstructive pulmonary disease (COPD) patients who are more protected from exacerbations with the use of an inhaled corticosteroid/long-acting β2 agonist (ICS/LABA) combination, compared with the use of LABA monotherapy.
Design: Post hoc cluster analysis of patients from two randomised clinical trials of salmeterol/fluticasone propionate (SFC) and salmeterol (SAL) that had primary endpoints of moderate/severe exacerbation rates.
Setting: Centres in North America.
Participants: 1543 COPD patients were studied.
Interventions: SFC 50/250 µg or SAL 50 µg, twice daily.
Primary and secondary outcome measures: The analysis identified clusters of COPD patients more responsive to SFC versus SAL with respect to the annual rate of moderate/severe exacerbations and compared their baseline clinical characteristics.
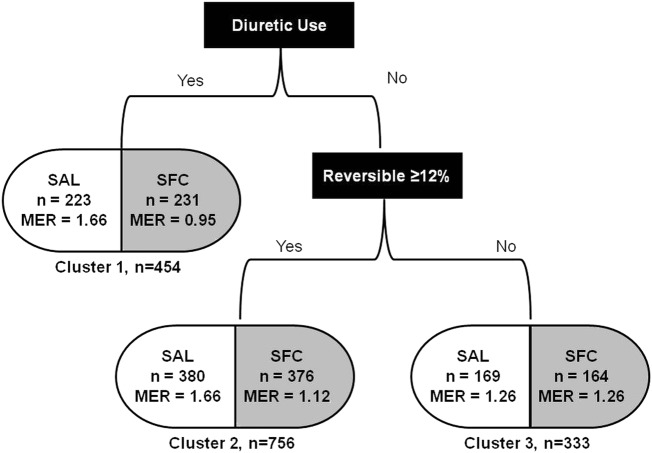
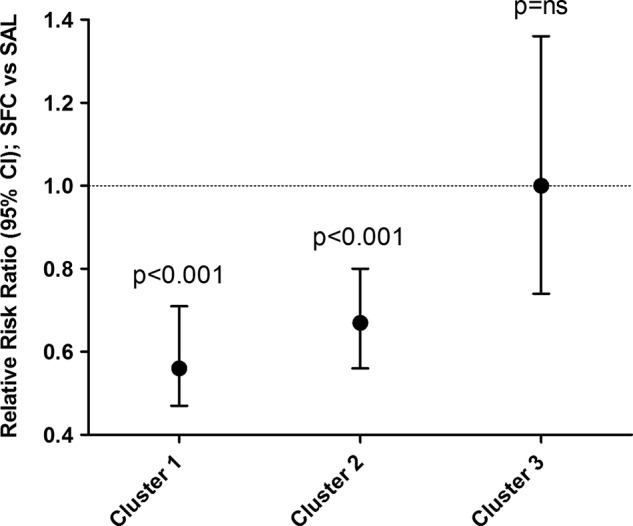
Results: Overall, SFC significantly reduced the annual rate of moderate/severe exacerbations as compared with SAL alone (rate ratio (RR)=0.701, p<0.001). Three-patient clusters were identified: COPD patients receiving diuretics (RR=0.56, p<0.001); patients not receiving diuretics but with forced expiratory volume in 1 s (FEV1) reversibility ≥12% (RR=0.67, p<0.001) exhibited a substantial reduction in the annual rate of moderate/severe exacerbations relative to SAL. A third cluster, consisting of patients not receiving diuretics and without FEV1 reversibility, demonstrated no difference for SFC versus SAL. Patients receiving diuretics had a significantly higher prevalence of comorbid cardiovascular disease.
Conclusions: COPD patients receiving diuretics and those not receiving diuretics but with FEV1 reversibility >12% at baseline were significantly more likely to experience a reduction in COPD-associated exacerbations with SFC versus SAL alone.
Trial registration: NCT00115492, NCT00144911.
Figures
References
-
- Global Initiative for Chronic Obstructive Lung Disease (GOLD) Global strategy for the diagnosis, management and prevention of COPD. 2011. http://www.goldcopd.org/ (accessed 1 Jun 2012). - PubMed
-
- Celli BR, Thomas NE, Anderson JA, et al. Effect of pharmacotherapy on rate of decline of lung function in chronic obstructive pulmonary disease: results from the TORCH study. Am J Respir Crit Care Med 2008;178:332–8 - PubMed
-
- Spencer S, Calverley PM, Burge PS, et al. Impact of preventing exacerbations on deterioration of health status in COPD. Eur Respir J 2004;23:698–702 - PubMed
-
- Agusti AG. COPD, a multicomponent disease: implications for management. Respir Med 2005;99:670–82 - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical