

Clinical evaluation of Rega 8: an updated genotypic interpretation system that significantly predicts HIV-therapy response
- PMID: 23613852
- PMCID: PMC3629176
- DOI: 10.1371/journal.pone.0061436
Clinical evaluation of Rega 8: an updated genotypic interpretation system that significantly predicts HIV-therapy response
Abstract
Introduction: Clinically evaluating genotypic interpretation systems is essential to provide optimal guidance in designing potent individualized HIV-regimens. This study aimed at investigating the ability of the latest Rega algorithm to predict virological response on a short and longer period.
Materials methods: 9231 treatment changes episodes were extracted from an integrated patient database. The virological response after 8, 24 and 48 weeks was dichotomized to success and failure. Success was defined as a viral load below 50 copies/ml or alternatively, a 2 log decrease from the baseline viral load at 8 weeks. The predictive ability of Rega version 8 was analysed in comparison with that of previous evaluated version Rega 5 and two other algorithms (ANRS v2011.05 and Stanford HIVdb v6.0.11). A logistic model based on the genotypic susceptibility score was used to predict virological response, and additionally, confounding factors were added to the model. Performance of the models was compared using the area under the ROC curve (AUC) and a Wilcoxon signed-rank test.
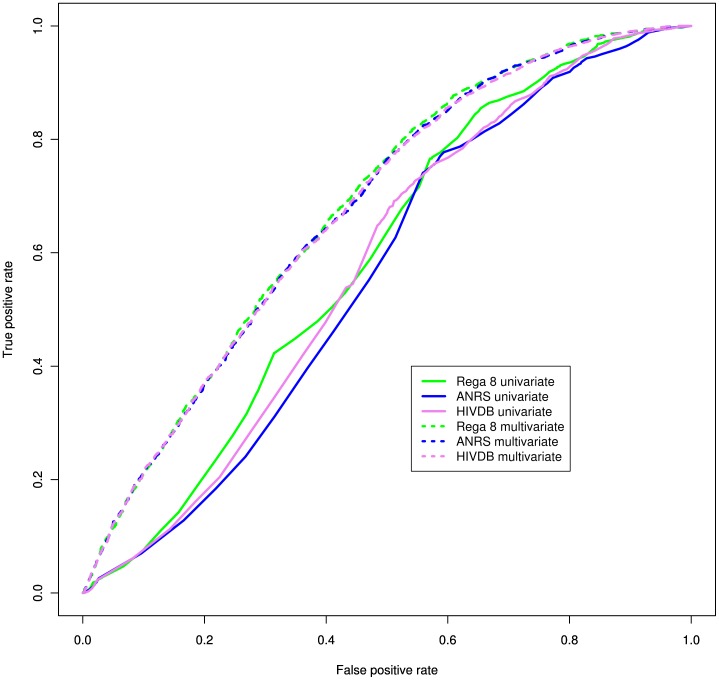
Results: Per unit increase of the GSS reported by Rega 8, the odds on having a successful therapy response on week 8 increased significantly by 81% (OR = 1.81, CI = [1.76-1.86]), on week 24 by 73% (OR = 1.73, CI = [1.69-1.78]) and on week 48 by 85% (OR = 1.85, CI = [1.80-1.91]). No significant differences in AUC were found between the performance of Rega 8 and Rega 5, ANRS v2011.05 and Stanford HIVdb v6.0.11, however Rega 8 had the highest sensitivity: 76.9%, 76.5% and 77.2% on 8, 24 and 48 weeks respectively. Inclusion of additional factors increased the performance significantly.
Conclusion: Rega 8 is a significant predictor for virological response with a better sensitivity than previously, and with rules for recently approved drugs. Additional variables should be taken into account to ensure an effective regimen.
Conflict of interest statement
Figures
Similar articles
-
Comparison of HIV-1 genotypic resistance test interpretation systems in predicting virological outcomes over time.PLoS One. 2010 Jul 9;5(7):e11505. doi: 10.1371/journal.pone.0011505. PLoS One. 2010. PMID: 20634893 Free PMC article.
-
Rules-based HIV-1 genotypic resistance interpretation systems predict 8 week and 24 week virological antiretroviral treatment outcome and benefit from drug potency weighting.J Antimicrob Chemother. 2009 Sep;64(3):616-24. doi: 10.1093/jac/dkp252. Epub 2009 Jul 19. J Antimicrob Chemother. 2009. PMID: 19620134
-
Baseline resistance and virological outcome in patients with virological failure who start a regimen containing abacavir: EuroSIDA study.Antivir Ther. 2004 Oct;9(5):787-800. Antivir Ther. 2004. PMID: 15535417
-
Study of the impact of HIV genotypic drug resistance testing on therapy efficacy.Verh K Acad Geneeskd Belg. 2001;63(5):447-73. Verh K Acad Geneeskd Belg. 2001. PMID: 11813503 Review.
-
Computer-Aided Optimization of Combined Anti-Retroviral Therapy for HIV: New Drugs, New Drug Targets and Drug Resistance.Curr HIV Res. 2016;14(2):101-9. doi: 10.2174/1570162x13666151029102254. Curr HIV Res. 2016. PMID: 26511342 Review.
Cited by
-
EPICE-HIV: An Epidemiologic Cost-Effectiveness Model for HIV Treatment.PLoS One. 2016 Feb 12;11(2):e0149007. doi: 10.1371/journal.pone.0149007. eCollection 2016. PLoS One. 2016. PMID: 26870960 Free PMC article.
-
Human Immunodeficiency Virus Drug Resistance: 2018 Recommendations of the International Antiviral Society-USA Panel.Clin Infect Dis. 2019 Jan 7;68(2):177-187. doi: 10.1093/cid/ciy463. Clin Infect Dis. 2019. PMID: 30052811 Free PMC article.
-
Drug resistance testing through remote genotyping and predicted treatment options in human immunodeficiency virus type 1 infected Tanzanian subjects failing first or second line antiretroviral therapy.PLoS One. 2017 Jun 5;12(6):e0178942. doi: 10.1371/journal.pone.0178942. eCollection 2017. PLoS One. 2017. PMID: 28582463 Free PMC article.
-
A new ensemble coevolution system for detecting HIV-1 protein coevolution.Biol Direct. 2015 Jan 7;10:1. doi: 10.1186/s13062-014-0031-8. Biol Direct. 2015. PMID: 25564011 Free PMC article.
-
Sub-Epidemics Explain Localized High Prevalence of Reduced Susceptibility to Rilpivirine in Treatment-Naive HIV-1-Infected Patients: Subtype and Geographic Compartmentalization of Baseline Resistance Mutations.AIDS Res Hum Retroviruses. 2016 May;32(5):427-33. doi: 10.1089/AID.2015.0095. Epub 2016 Jan 29. AIDS Res Hum Retroviruses. 2016. PMID: 26651266 Free PMC article.
References
-
- Mocroft A, Vella S, Benfield TL, Chiesi A, Miller V, et al. (1998) Changing patterns of mortality across Europe in patients infected with HIV-1. EuroSIDA Study Group. Lancet 352: 1725–30. - PubMed
-
- Thompson MA, Aberg JA, Cahn P, Montaner JSG, Rizzardini G, et al. (2010) Antiretroviral treatment of adult HIV infection: 2010 recommendations of the International AIDS Society-USA panel. JAMA : the journal of the American Medical Association 304: 321–33. - PubMed
-
- Wilson LE, Gallant JE (2009) HIV/AIDS: the management of treatment-experienced HIV-infected patients: new drugs and drug combinations. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 48: 214–21. - PubMed
-
- Vercauteren J, Vandamme AM (2006) Algorithms for the interpretation of HIV-1 genotypic drug resistance information. Antiviral research 71: 335–42. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
