

A Randomized Controlled Trial about the Levels of Radiation Exposure Depends on the Use of Collimation C-arm Fluoroscopic-guided Medial Branch Block
- PMID: 23614076
- PMCID: PMC3629341
- DOI: 10.3344/kjp.2013.26.2.148
A Randomized Controlled Trial about the Levels of Radiation Exposure Depends on the Use of Collimation C-arm Fluoroscopic-guided Medial Branch Block
Abstract
Background: C-arm fluoroscope has been widely used to promote more effective pain management; however, unwanted radiation exposure for operators is inevitable. We prospectively investigated the differences in radiation exposure related to collimation in Medial Branch Block (MBB).
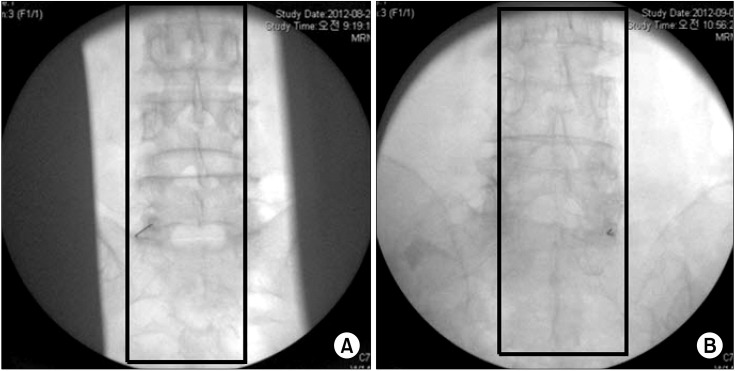
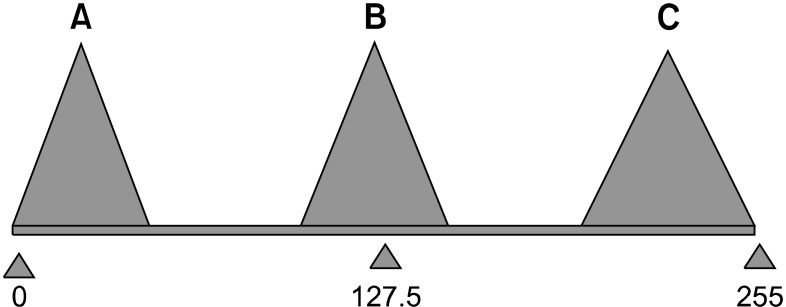
Methods: This study was a randomized controlled trial of 62 MBBs at L3, 4 and 5. After the patient was laid in the prone position on the operating table, MBB was conducted and only AP projections of the fluoroscope were used. Based on a concealed random number table, MBB was performed with (collimation group) and without (control group) collimation. The data on the patient's age, height, gender, laterality (right/left), radiation absorbed dose (RAD), exposure time, distance from the center of the field to the operator, and effective dose (ED) at the side of the table and at the operator's chest were collected. The brightness of the fluoroscopic image was evaluated with histogram in Photoshop.
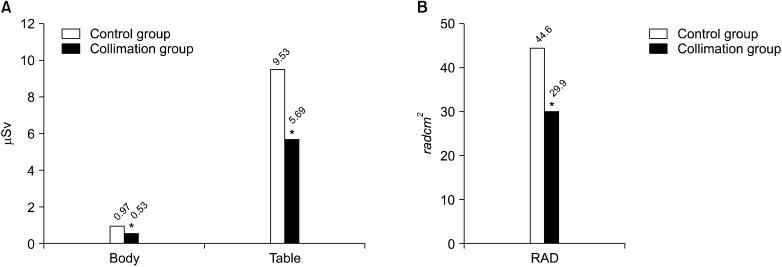
Results: There were no significant differences in age, height, weight, male to female ratio, laterality, time, distance and brightness of fluoroscopic image. The area of the fluoroscopic image with collimation was 67% of the conventional image. The RAD (29.9 ± 13.0, P = 0.001) and the ED at the left chest of the operators (0.53 ± 0.71, P = 0.042) and beside the table (5.69 ± 4.6, P = 0.025) in collimation group were lower than that of the control group (44.6 ± 19.0, 0.97 ± 0.92, and 9.53 ± 8.16), resepectively.
Conclusions: Collimation reduced radiation exposure and maintained the image quality. Therefore, the proper use of collimation will be beneficial to both patients and operators.
Keywords: collimation; image quality; radiation absorbed dose; radiation exposure.
Figures

Similar articles
-
The Radiation Exposure of Radiographer Related to the Location in C-arm Fluoroscopy-guided Pain Interventions.Korean J Pain. 2014 Apr;27(2):162-7. doi: 10.3344/kjp.2014.27.2.162. Epub 2014 Mar 28. Korean J Pain. 2014. PMID: 24748945 Free PMC article.
-
Radiation Exposure of the Hand and Chest during C-arm Fluoroscopy-Guided Procedures.Korean J Pain. 2013 Jan;26(1):51-6. doi: 10.3344/kjp.2013.26.1.51. Epub 2013 Jan 4. Korean J Pain. 2013. PMID: 23342208 Free PMC article.
-
Comparison of Intravascular Uptake and Technical Ease Between Anteroposterior and Oblique Views During Lumbar Medial Branch Block.Pain Physician. 2022 Oct;25(7):E969-E975. Pain Physician. 2022. PMID: 36288582 Clinical Trial.
-
Techniques to reduce radiation and contrast volume during EVAR.J Cardiovasc Surg (Torino). 2014 Apr;55(2 Suppl 1):123-31. J Cardiovasc Surg (Torino). 2014. PMID: 24796905 Review.
-
Occupational radiation doses to operators performing cardiac catheterization procedures.Health Phys. 2008 Mar;94(3):211-27. doi: 10.1097/01.HP.0000290614.76386.35. Health Phys. 2008. PMID: 18301095 Review.
Cited by
-
Radiation safety: a focus on lead aprons and thyroid shields in interventional pain management.Korean J Pain. 2018 Oct;31(4):244-252. doi: 10.3344/kjp.2018.31.4.244. Epub 2018 Oct 1. Korean J Pain. 2018. PMID: 30310549 Free PMC article. Review.
-
How Effective Are Radiation Reducing Gloves in C-arm Fluoroscopy-guided Pain Interventions?Korean J Pain. 2014 Apr;27(2):145-51. doi: 10.3344/kjp.2014.27.2.145. Epub 2014 Mar 28. Korean J Pain. 2014. PMID: 24748943 Free PMC article.
-
Radiation safety for pain physicians: technique or equipment.Korean J Pain. 2014 Apr;27(2):101-2. doi: 10.3344/kjp.2014.27.2.101. Epub 2014 Mar 28. Korean J Pain. 2014. PMID: 24748936 Free PMC article. No abstract available.
-
Evaluation of protective equipment for the reduction of radiation exposure to physicians performing fluoroscopically guided lumbar transforaminal epidural steroid injections: A randomized controlled trial.Medicine (Baltimore). 2020 Jul 31;99(31):e21424. doi: 10.1097/MD.0000000000021424. Medicine (Baltimore). 2020. PMID: 32756146 Free PMC article. Clinical Trial.
-
The Radiation Exposure of Radiographer Related to the Location in C-arm Fluoroscopy-guided Pain Interventions.Korean J Pain. 2014 Apr;27(2):162-7. doi: 10.3344/kjp.2014.27.2.162. Epub 2014 Mar 28. Korean J Pain. 2014. PMID: 24748945 Free PMC article.
References
-
- Fink GE. Radiation safety in fluoroscopy for neuraxial injections. AANA J. 2009;77:265–269. - PubMed
-
- Singer G. Occupational radiation exposure to the surgeon. J Am Acad Orthop Surg. 2005;13:69–76. - PubMed
-
- Miller DL, Vañó E, Bartal G, Balter S, Dixon R, Padovani R, et al. Occupational radiation protection in interventional radiology: a joint guideline of the Cardiovascular and Interventional Radiology Society of Europe and the Society of Interventional Radiology. J Vasc Interv Radiol. 2010;21:607–615. - PubMed
-
- Le Heron J, Padovani R, Smith I, Czarwinski R. Radiation protection of medical staff. Eur J Radiol. 2010;76:20–23. - PubMed
-
- Killewich LA, Singleton TA. Governmental regulations and radiation exposure. J Vasc Surg. 2011;53:44S–46S. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources