

Physician-pharmacist co-management and 24-hour blood pressure control
- PMID: 23614849
- PMCID: PMC3641686
- DOI: 10.1111/jch.12077
Physician-pharmacist co-management and 24-hour blood pressure control
Abstract
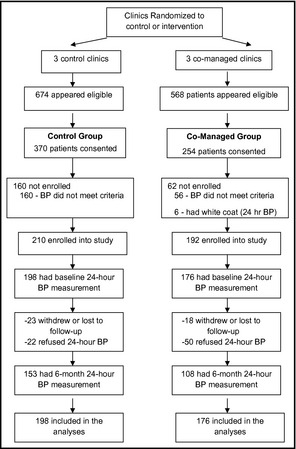
The objectives of this study were to compare indices of 24-hour blood pressure (BP) following a physician-pharmacist collaborative intervention and to describe the associated changes in antihypertensive medications. This was a secondary analysis of a prospective, cluster-randomized clinical trial conducted in 6 family medicine clinics randomized to co-managed (n=3 clinics, 176 patients) or control (n=3 clinics, 198 patients) groups. Mean ambulatory systolic BP (SBP) was significantly lower in the co-managed vs the control group: daytime BP 122.8 mm Hg vs 134.4 mm Hg (P<.001); nighttime SBP 114.8 mm Hg vs 123.7 mm Hg (P<.001); and 24-hour SBP 120.4 mm Hg vs 131.8 mm Hg (P<.001), respectively. Significantly more drug changes were made in the co-managed than in the control group (2.7 vs 1.1 changes per patient, P<.001), and there was greater diuretic use in co-managed patients (79.6% vs 62.6%, P<.001). Ambulatory BPs were significantly lower for the patients who had a diuretic added during the first month compared with those who never had a diuretic added (P<.01). Physician-pharmacist co-management significantly improved ambulatory BP compared with the control group. Antihypertensive drug therapy was intensified much more for patients in the co-managed group.
© 2013 Wiley Periodicals, Inc.
Figures
References
-
- Yoon PW, Gillespie CD, George MG, Wall HK. Control of hypertension among adults–national health and nutrition examination survey, United States, 2005–2008. MMWR Morb Mortal Wkly Rep. 2012;61(suppl):19–25. - PubMed
-
- Wolf‐Maier K, Cooper RS, Banegas JR, et al. Hypertension prevalence and blood pressure levels in 6 European countries, Canada, and the United States. JAMA. 2003;289:2363–2369. - PubMed
-
- Lloyd‐Jones D, Adams RJ, Brown TM, et al. Executive summary: heart disease and stroke statistics–2010 update: a report from the American Heart Association. Circulation. 2010;121:948–954. - PubMed
-
- Heidenreich PA, Trogdon JG, Khavjou OA, et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 2011;123:933–944. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
