

No independent association of serum phosphorus with risk for death or progression to end-stage renal disease in a large screen for chronic kidney disease
- PMID: 23615501
- PMCID: PMC4103660
- DOI: 10.1038/ki.2013.145
No independent association of serum phosphorus with risk for death or progression to end-stage renal disease in a large screen for chronic kidney disease
Abstract
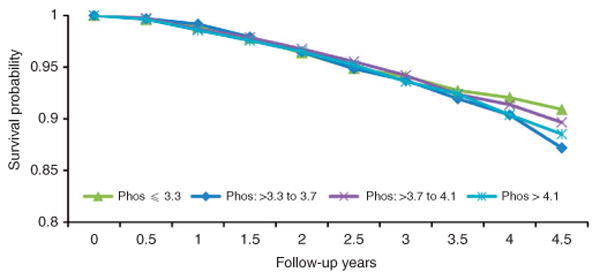
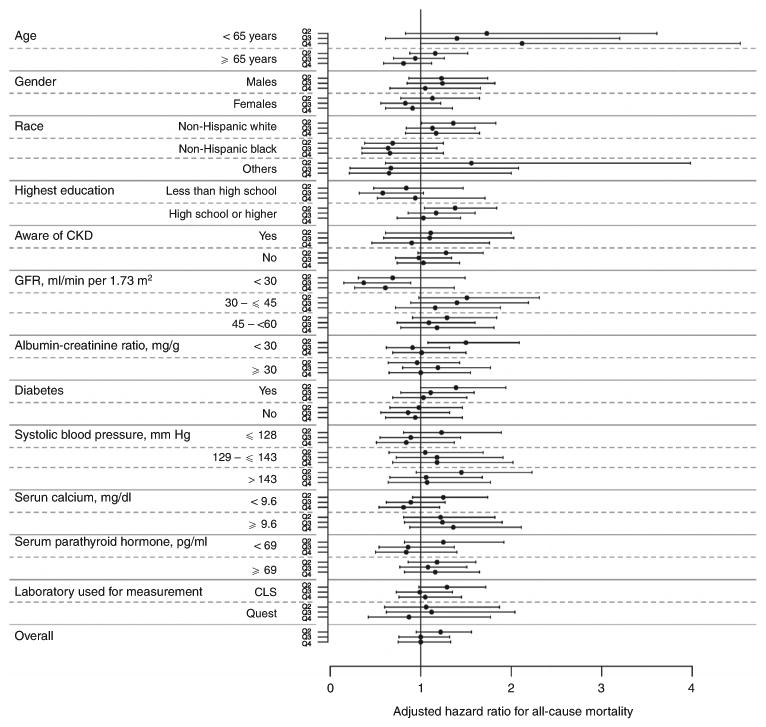
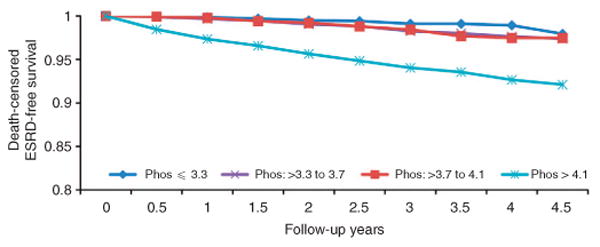
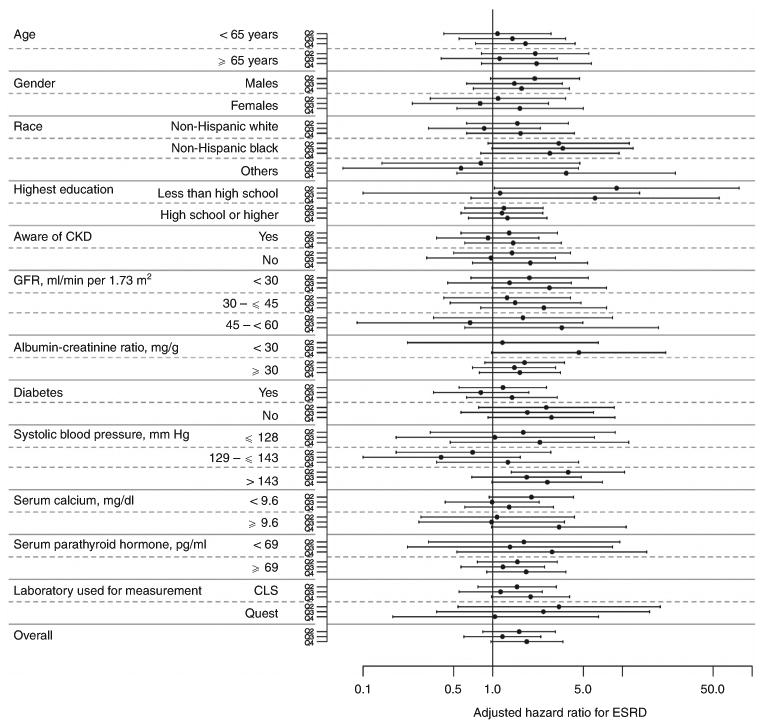
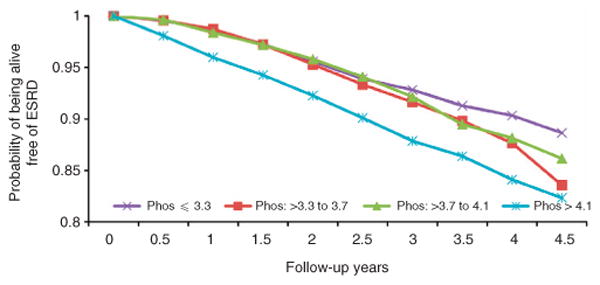
Whether higher serum phosphorus levels are associated with a higher risk for death and/or progression of chronic kidney disease (CKD) is not well established, and whether the association is confounded by access and barriers to care is unknown. To answer these questions, data of 10,672 individuals identified to have CKD (estimated glomerular filtration rate <60 ml/min per 1.73 m(2)) from those participating in a community-based screening program were analyzed. Over a median follow-up of 2.3 years, there was no association between quartiles of serum phosphorus and all-cause mortality (adjusted hazards ratio for serum phosphorus over 3.3 to 3.7, over 3.7 to 4.1, and over 4.1 mg/dl, respectively: 1.22 (0.95-1.56), 1.00 (0.76-1.32), and 1.00 (0.75-1.33); reference, serum phosphorus of 3.3 mg/dl and below). Individuals in the highest quartile for serum phosphorus had a significantly higher risk for progression to end-stage renal disease (ESRD) (unadjusted hazards ratio, 6.72 (4.16-10.85)); however, the risk became nonsignificant on adjustment for potential confounders. There was no appreciable change in hazards ratio with inclusion of variables related to access and barriers to care. Additional analyses in subgroups based on 12 different variables yielded similar negative associations. Thus, in the largest cohort of individuals with early-stage CKD to date, we could not validate an independent association of serum phosphorus with risk for death or progression to ESRD.
Conflict of interest statement
All the other authors declared no competing interests.
Figures
Comment in
-
Chronic kidney disease: Does serum phosphate predict death and ESRD in CKD patients?Nat Rev Nephrol. 2013 Aug;9(8):438-9. doi: 10.1038/nrneph.2013.128. Epub 2013 Jul 2. Nat Rev Nephrol. 2013. PMID: 23820817 No abstract available.
-
Serum phosphorus in people with chronic kidney disease: you are what you eat.Kidney Int. 2013 Nov;84(5):871-3. doi: 10.1038/ki.2013.258. Kidney Int. 2013. PMID: 24172733
References
-
- Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305. - PubMed
-
- Keith DS, Nichols GA, Gullion CM, et al. Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch Intern Med. 2004;164:659–663. - PubMed
-
- Holtkamp FA, de Zeeuw D, de Graeff PA, et al. Albuminuria and blood pressure, independent targets for cardioprotective therapy in patients with diabetes and nephropathy: a post hoc analysis of the combined RENAAL and IDNT trials. Eur Heart J. 2011;32:1493–1499. - PubMed
-
- Block GA. Therapeutic interventions for chronic kidney disease-mineral and bone disorders: focus on mortality. Curr Opin Nephrol Hypertens. 2011;20:376–381. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
