

Conductive hearing loss induced by experimental middle-ear effusion in a chinchilla model reveals impaired tympanic membrane-coupled ossicular chain movement
- PMID: 23615802
- PMCID: PMC3705087
- DOI: 10.1007/s10162-013-0388-x
Conductive hearing loss induced by experimental middle-ear effusion in a chinchilla model reveals impaired tympanic membrane-coupled ossicular chain movement
Erratum in
- J Assoc Res Otolaryngol. 2013 Aug;14(4):465. Tollin, Daniel [corrected to Tollin, Daniel J]
Abstract
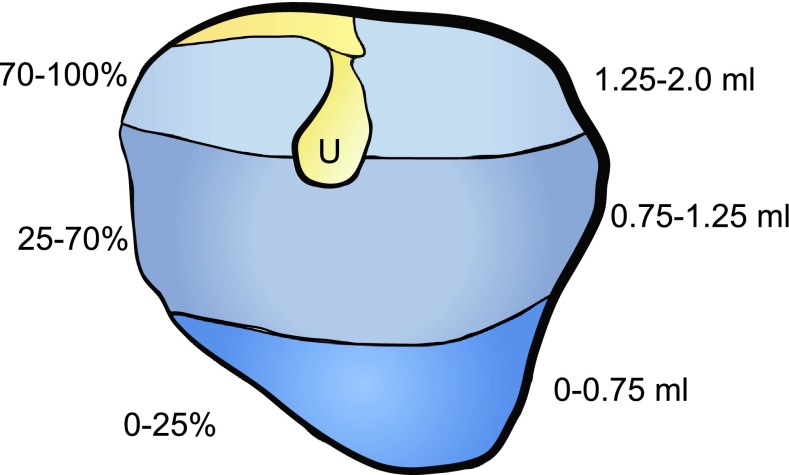
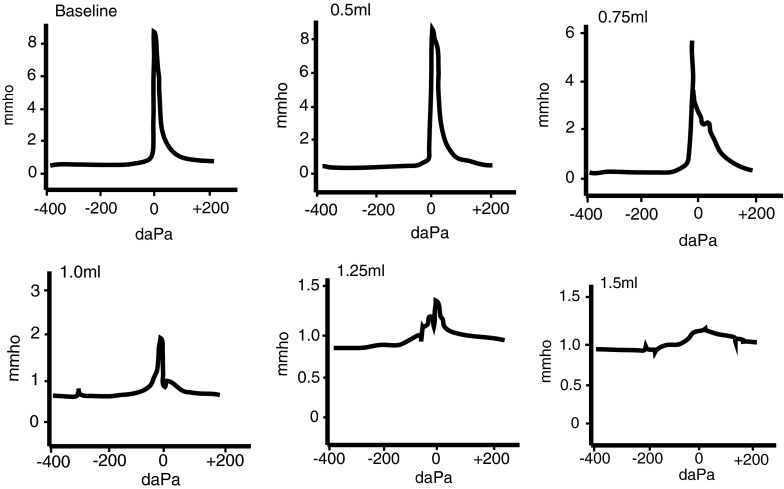
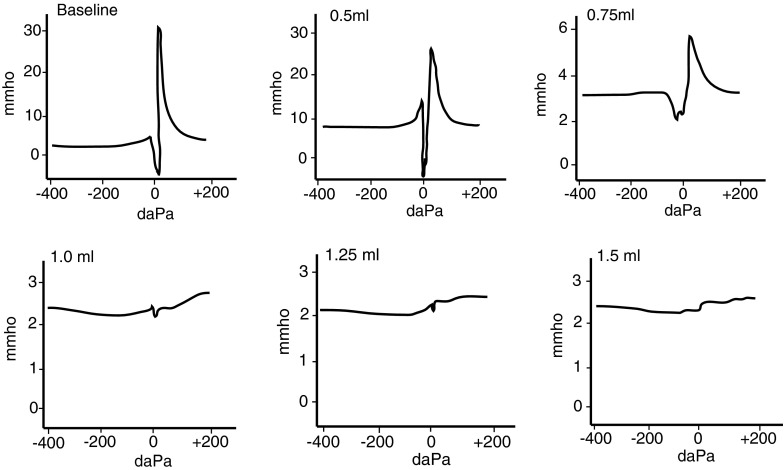
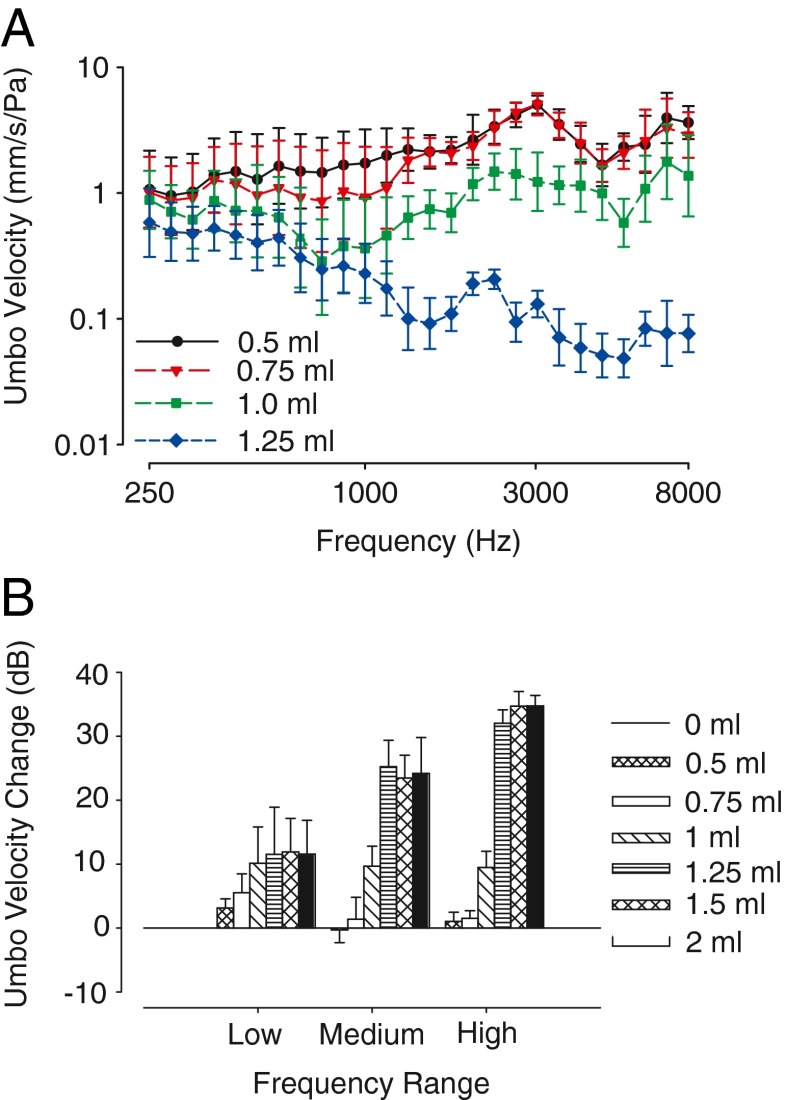
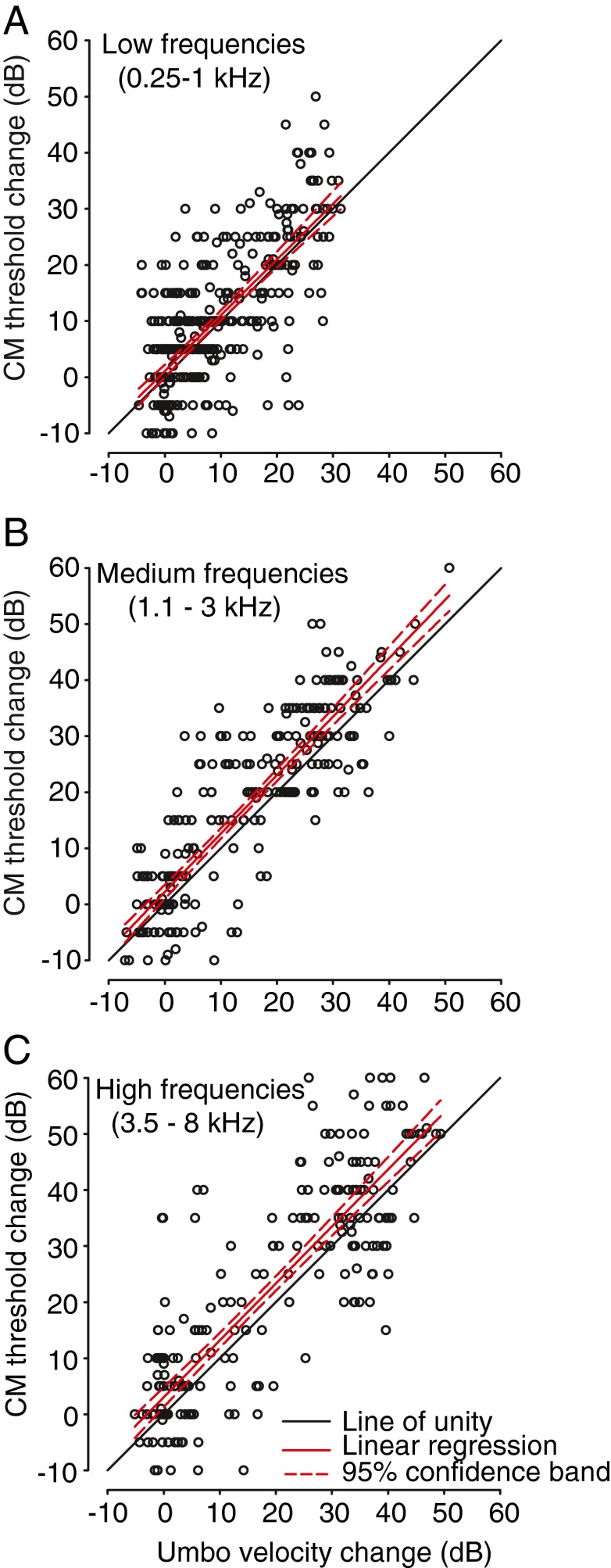
Otitis media with effusion (OME) occurs when fluid collects in the middle-ear space behind the tympanic membrane (TM). As a result of this effusion, sounds can become attenuated by as much as 30-40 dB, causing a conductive hearing loss (CHL). However, the exact mechanical cause of the hearing loss remains unclear. Possible causes can include altered compliance of the TM, inefficient movement of the ossicular chain, decreased compliance of the oval window-stapes footplate complex, or altered input to the oval and round window due to conduction of sound energy through middle-ear fluid. Here, we studied the contribution of TM motion and umbo velocity to a CHL caused by middle-ear effusion. Using the chinchilla as an animal model, umbo velocity (V U) and cochlear microphonic (CM) responses were measured simultaneously using sinusoidal tone pip stimuli (125 Hz-12 kHz) before and after filling the middle ear with different volumes (0.5-2.0 mL) of silicone oil (viscosity, 3.5 Poise). Concurrent increases in CM thresholds and decreases in umbo velocity were noted after the middle ear was filled with 1.0 mL or more of fluid. Across animals, completely filling the middle ear with fluid caused 20-40-dB increases in CM thresholds and 15-35-dB attenuations in umbo velocity. Clinic-standard 226-Hz tympanometry was insensitive to fluid-associated changes in CM thresholds until virtually the entire middle-ear cavity had been filled (approximately >1.5 mL). The changes in umbo velocity, CM thresholds, and tympanometry due to experimentally induced OME suggest CHL arises primarily as a result of impaired TM mobility and TM-coupled umbo motion plus additional mechanisms within the middle ear.
Figures

References
-
- Bennett MJ, Weatherby LA. Newborn acoustic reflexes to noise and pure-tone signals. J Speech Hear Res. 1982;25:383–387. - PubMed
-
- Bluestone CD, Klein JO (eds) (1995) Definitions, terminology, and classification. In: Otitis media in infants and children, 2nd edn. W.B. Saunders Co., Philadelphia p 1–3
-
- Browning GC, Granich M. Surgical anatomy of the temporal bone in the chinchilla. Ann Otol Rhinol Laryngol. 1978;87:875–882. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
