

The midbrain to pons ratio: a simple and specific MRI sign of progressive supranuclear palsy
- PMID: 23616165
- PMCID: PMC3908351
- DOI: 10.1212/WNL.0b013e318292a2d2
The midbrain to pons ratio: a simple and specific MRI sign of progressive supranuclear palsy
Abstract
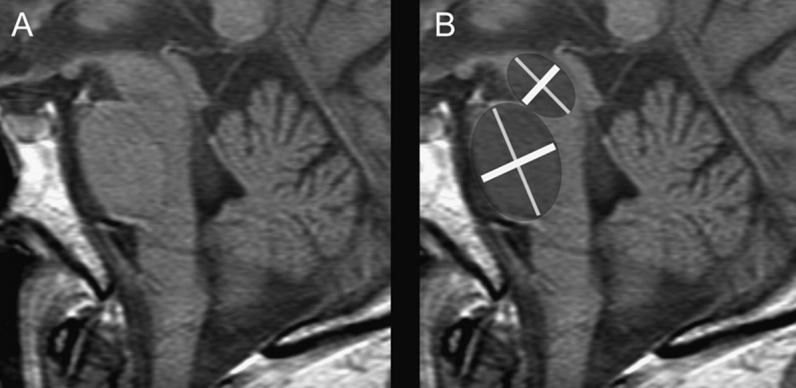
Objectives: MRI-based measurements used to diagnose progressive supranuclear palsy (PSP) typically lack pathologic verification and are not easy to use routinely. We aimed to develop in histologically proven disease a simple measure of the midbrain and pons on sagittal MRI to identify PSP.
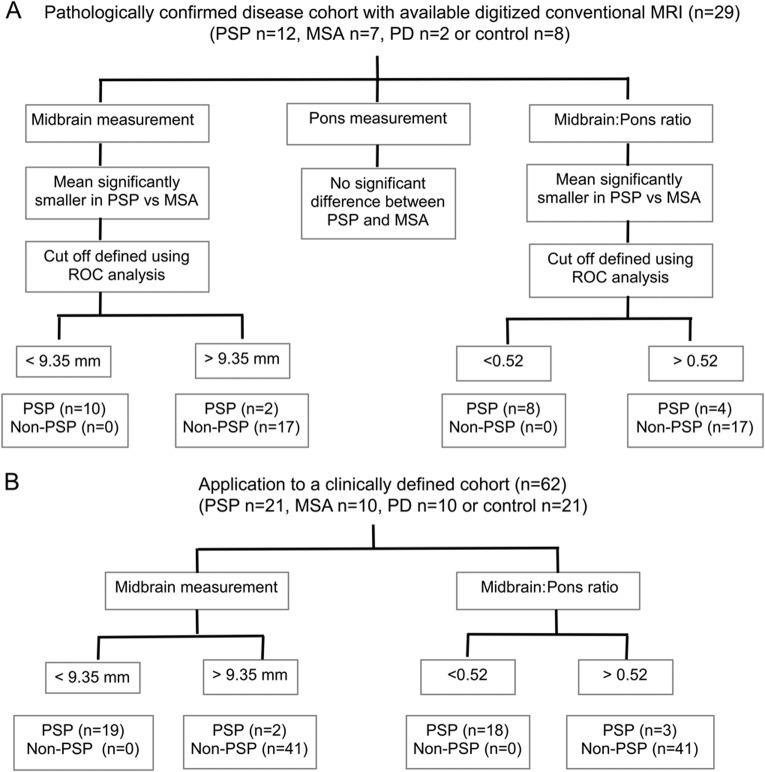
Methods: Measurements of the midbrain and pontine base on midsagittal T1-weighted MRI were performed in confirmed PSP (n = 12), Parkinson disease (n = 2), and multiple system atrophy (MSA) (n = 7), and in controls (n = 8). Using receiver operating characteristic curve analysis, cutoff values were applied to a clinically diagnosed cohort of 62 subjects that included PSP (n = 21), Parkinson disease (n = 10), MSA (n = 10), and controls (n = 21).
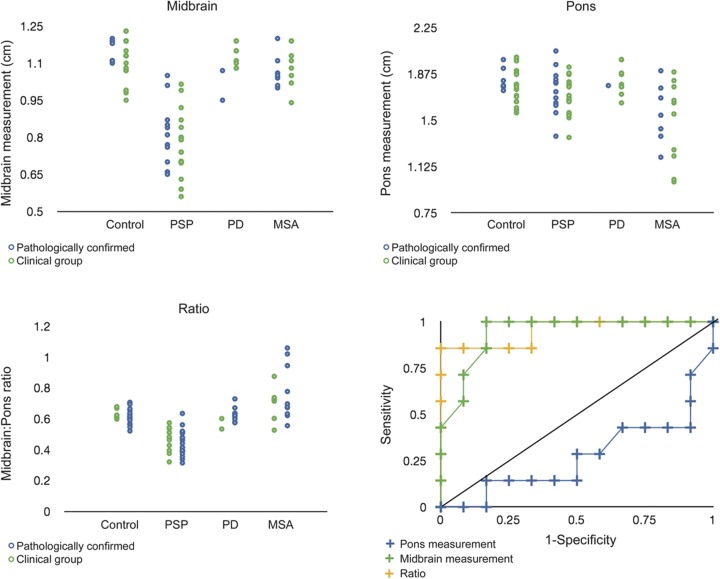
Results: The mean midbrain measurement of 8.1 mm was reduced in PSP (p < 0.001) with reduction in the midbrain to pons ratio (PSP smaller than MSA; p < 0.001). In controls, the mean midbrain ratio was approximately two-thirds of the pontine base, in PSP it was <52%, and in MSA the ratio was greater than two-thirds. A midbrain measurement of <9.35 mm and ratio of 0.52 had 100% specificity for PSP. In the clinically defined group, 19 of 21 PSP cases (90.5%) had a midbrain measurement of <9.35 mm.
Conclusions: We have developed a simple and reliable measurement in pathologically confirmed disease based on the topography of atrophy in PSP with high sensitivity and specificity that may be a useful tool in the clinic.
Figures
Comment in
-
The midbrain to pons ratio: a simple and specific MRI sign of progressive supranuclear palsy.Neurology. 2013 Dec 10;81(24):2147. doi: 10.1212/01.WNL.0000437347.92583.fc. Neurology. 2013. PMID: 24323440 No abstract available.
References
-
- Hughes AJ, Daniel SE, Ben-Shlomo Y, Lees AJ. The accuracy of diagnosis of parkinsonian syndromes in a specialist movement disorder service. Brain 2002;125:861–870 - PubMed
-
- Massey LA, Micallef C, Paviour DC, et al. Conventional magnetic resonance imaging in confirmed progressive supranuclear palsy and multiple system atrophy. Mov Disord 2012;27:1754–1762 - PubMed
-
- Asato R, Akiguchi I, Masunaga S, Hashimoto N. Magnetic resonance imaging distinguishes progressive supranuclear palsy from multiple system atrophy. J Neural Transm 2000;107:1427–1436 - PubMed
-
- Kato N, Arai K, Hattori T. Study of the rostral midbrain atrophy in progressive supranuclear palsy. J Neurol Sci 2003;210:57–60 - PubMed
-
- Oba H, Yagishita A, Terada H, et al. New and reliable MRI diagnosis for progressive supranuclear palsy. Neurology 2005;64:2050–2055 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous