

Myocardial infarction and individual nonsteroidal anti-inflammatory drugs meta-analysis of observational studies
- PMID: 23616423
- PMCID: PMC3749466
- DOI: 10.1002/pds.3437
Myocardial infarction and individual nonsteroidal anti-inflammatory drugs meta-analysis of observational studies
Abstract
Objective: To conduct a systematic review of observational studies on the risk of acute myocardial infarction (AMI) with use of individual nonsteroidal anti-inflammatory drugs (NSAIDs).
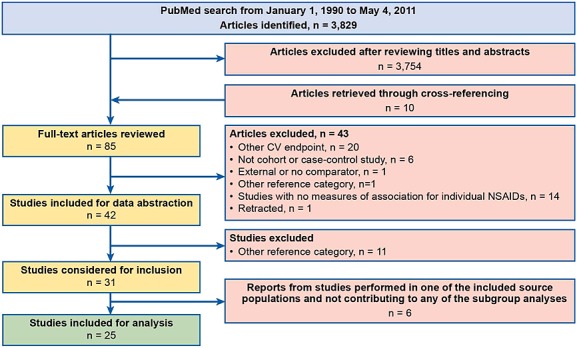
Methods: A search of Medline (PubMed) for observational studies published from 1990 to 2011 identified 3829 articles; 31 reported relative risk (RR) of AMI with use of individual NSAIDs versus nonuse of NSAIDs. Information abstracted in a standardized form from 25 publications was used for the meta-analysis on 18 independent study populations.
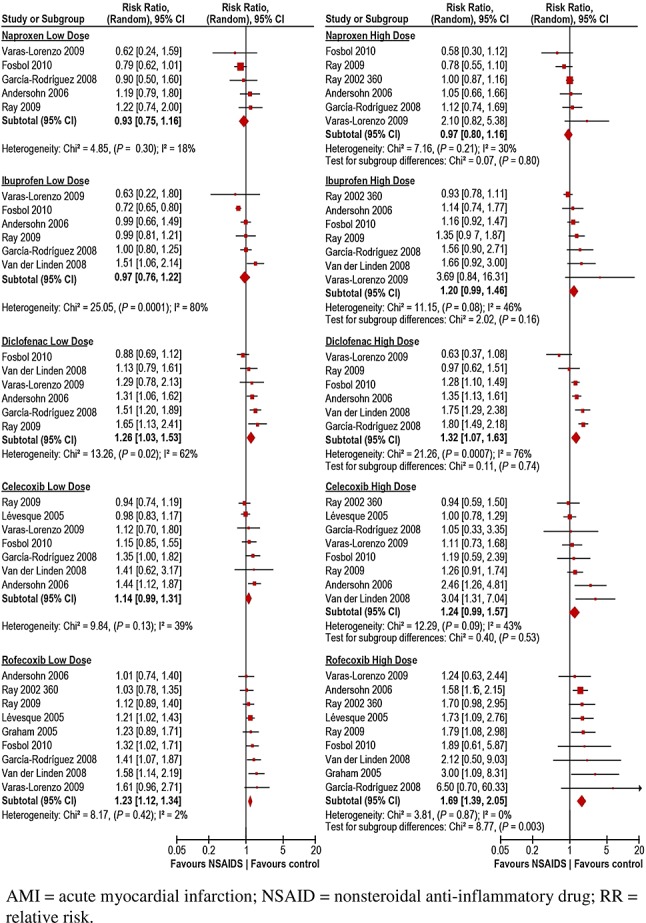
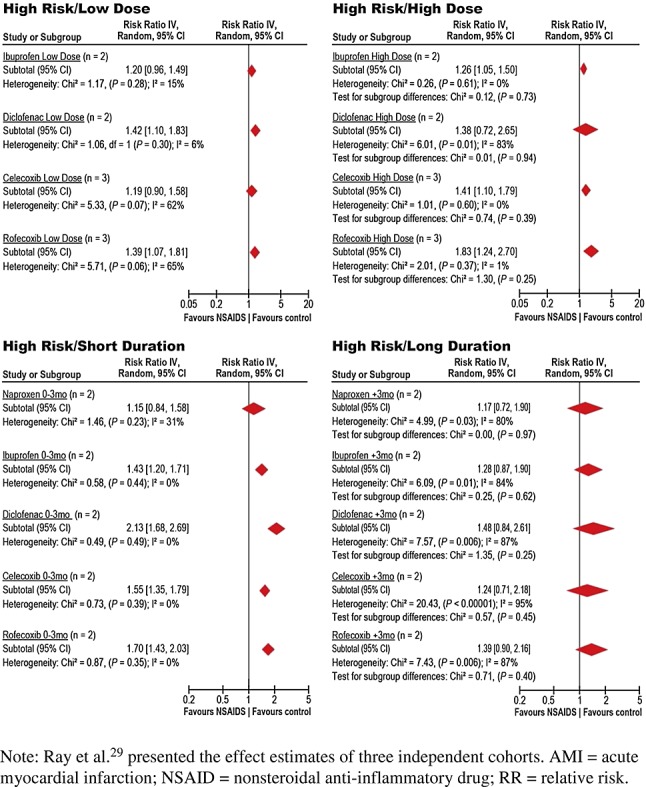
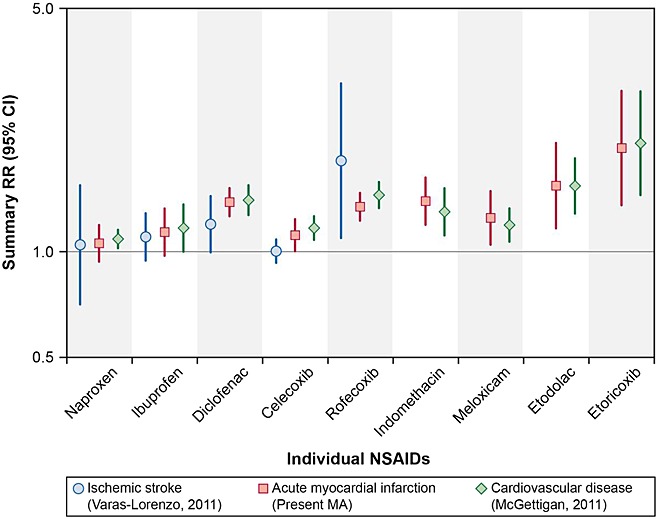
Results: Random-effects RR (95% confidence interval (CI)) was lowest for naproxen 1.06 (0.94–1.20), followed by celecoxib 1.12 (1.00–1.24), ibuprofen 1.14 (0.98–1.31), meloxicam 1.25 (1.04–1.49), rofecoxib 1.34 (1.22–1.48), diclofenac 1.38 (1.26–1.52), indometacin 1.40 (1.21–1.62), etodolac 1.55 (1.16–2.06), and etoricoxib 1.97 (1.35–2.89). Heterogeneity between studies was present. For new users, RRs (95% CIs) were for naproxen, 0.85 (0.73–1.00); ibuprofen, 1.20 (0.97–1.48); celecoxib, 1.23 (1.00–1.52); diclofenac, 1.41 (1.08–1.86); and rofecoxib, 1.43 (1.21–1.66).Except for naproxen, higher risk was generally associated with higher doses, as defined in each study, overall and in patients with prior coronary heart disease. Low and high doses of diclofenac and rofecoxib were associated with high risk of AMI, with dose–response relationship for rofecoxib. In patients with prior coronary heart disease, except for naproxen, duration of use ≤3 months was associated with an increased risk of AMI.
Conclusions: Most frequently NSAIDs used in clinical practice, except naproxen, are associated with an increased risk of AMI at high doses or in persons with diagnosed coronary heart disease. For diclofenac and rofecoxib, the risk was increased at low and high doses.
Figures
Comment in
-
Diclofenac: increase of myocardial infarctions at low doses?Pharmacoepidemiol Drug Saf. 2014 Mar;23(3):326-8. doi: 10.1002/pds.3564. Pharmacoepidemiol Drug Saf. 2014. PMID: 24596323 No abstract available.
-
Response to the letter to the editor entitled "diclofenac: increase of myocardial infarctions at low doses?" (PDS 13-0441) authored by K Brune.Pharmacoepidemiol Drug Saf. 2014 Mar;23(3):329-30. doi: 10.1002/pds.3563. Pharmacoepidemiol Drug Saf. 2014. PMID: 24596324 No abstract available.
References
-
- Bombardier C, Laine L, Reicin A, et al. Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. VIGOR Study Group. N Engl J Med. 2000;343:1520–8. 2 p following 8. DOI: 10.1056/NEJM200011233432103. - DOI - PubMed
-
- Bresalier RS, Sandler RS, Quan H, et al. Cardiovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. N Engl J Med. 2005;352:1092–102. DOI: 10.1056/NEJMoa050493. - DOI - PubMed
-
- Solomon SD, McMurray JJ, Pfeffer MA, et al. Cardiovascular risk associated with celecoxib in a clinical trial for colorectal adenoma prevention. N Engl J Med. 2005;352:1071–80. DOI: 10.1056/NEJMoa050405. - DOI - PubMed
-
- Hernández-Díaz S, Varas-Lorenzo C, García Rodríguez LA. Non-steroidal antiinflammatory drugs and the risk of acute myocardial infarction. Basic Clin Pharmacol Toxicol. 2006;98:266–74. DOI: 10.1111/j.1742-7843.2006.pto_302.x. - DOI - PubMed
-
- Kearney PM, Baigent C, Godwin J, Halls H, Emberson JR, Patrono C. Do selective cyclo-oxygenase-2 inhibitors and traditional non-steroidal anti-inflammatory drugs increase the risk of atherothrombosis? Meta-analysis of randomised trials. BMJ. 2006;332:1302–8. DOI: 10.1136/bmj.332.7553.1302. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
