

Mimics and chameleons in motor neurone disease
- PMID: 23616620
- PMCID: PMC3664389
- DOI: 10.1136/practneurol-2013-000557
Mimics and chameleons in motor neurone disease
Abstract
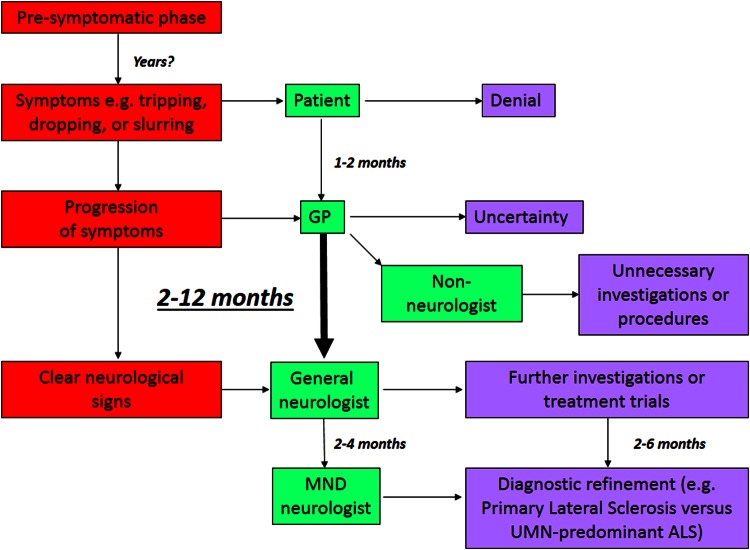
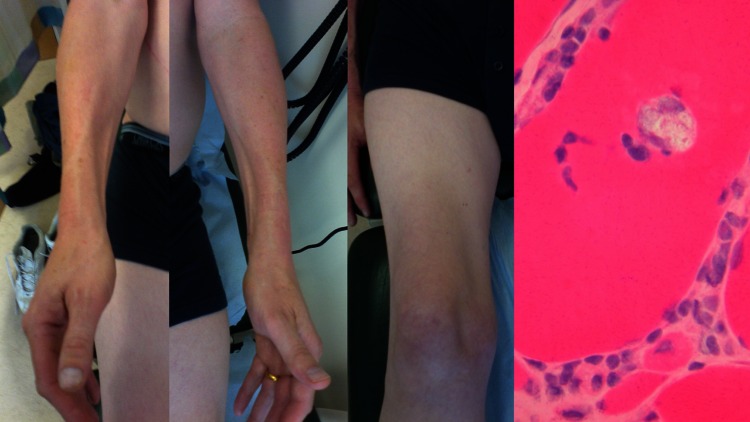
The progression of motor neurone disease (MND) is currently irreversible, and the grave implications of diagnosis naturally fuels concern among neurologists over missing a potential mimic disorder. There is no diagnostic test for MND but in reality there are few plausible mimics in routine clinical practice. In the presence of a progressive pure motor disorder, signs such as florid fasciculations, bilateral tongue wasting, the 'split hand', head drop, emotionality, and cognitive or behavioural impairment carry high positive predictive value. MND is clinically heterogeneous, however, with some important chameleon-like presentations and considerable variation in clinical course. Lack of confidence about the scope of such variation, or an approach to diagnosis emphasising investigations over clinical common sense, has the potential to exacerbate diagnostic delay in MND and impede timely planning of the care which is essential to maximising quality of life.
Keywords: MOTOR NEURON DISEASE.
Figures





References
-
- Matthews WB. Practical neurology. 2nd edn Philadelphia: F.A. Davis Company, 1970
-
- Mitchell JD, Callagher P, Gardham J, et al. Timelines in the diagnostic evaluation of people with suspected amyotrophic lateral sclerosis (ALS)/motor neuron disease (MND)—a 20-year review: Can we do better? Amyotroph Lateral Scler 2010;11:537–41 - PubMed
-
- Kiernan MC, Vucic S, Cheah BC, et al. Amyotrophic lateral sclerosis. Lancet 2011;377:942–55 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources