

Prevalence of self-reported spondyloarthritis features in a cohort of patients with inflammatory bowel disease
- PMID: 23616957
- PMCID: PMC3742476
- DOI: 10.1155/2013/139702
Prevalence of self-reported spondyloarthritis features in a cohort of patients with inflammatory bowel disease
Abstract
Background: Musculoskeletal symptoms belonging to the spectrum of 'seronegative spondyloarthritis' (SpA) are the most common extraintestinal manifestations in patients with inflammatory bowel disease (IBD) and may lead to important disease burden. Patients with suspected SpA should be referred to a rheumatologist for further evaluation.
Objective: To investigate the self-reported prevalence of musculoskeletal SpA features in a cohort of patients with IBD and to compare this with actual referrals to a rheumatologist.
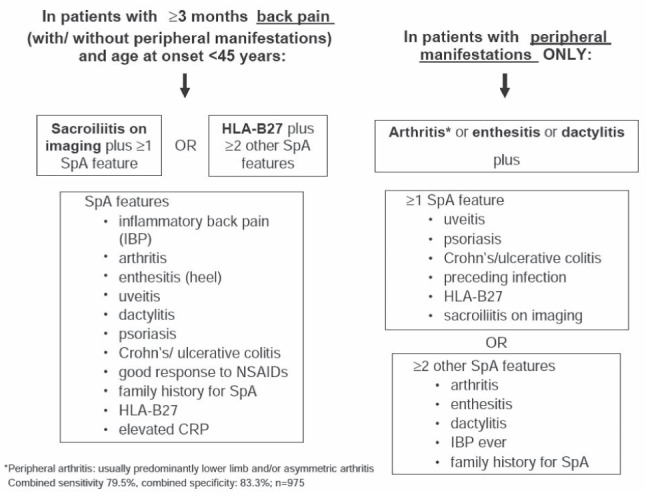
Methods: Consecutive patients with IBD visiting the outpatient clinic were interviewed by a trained research nurse about possible SpA features using a standardized questionnaire regarding the presence or history of inflammatory back pain, peripheral arthritis, enthesitis, dactylitis, psoriasis, uveitis and response to nonsteroidal anti-inflammatory drugs. All patient files were verified for previous visits to a rheumatologist and any rheumatic diagnosis.
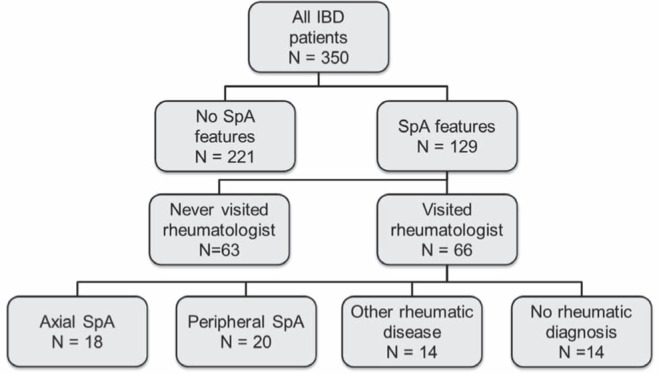
Results: At least one musculoskeletal SpA feature was reported by 129 of 350 (36.9%) patients. No significant differences between patients with Crohn disease and ulcerative colitis were found. Review of medical records showed that 66 (51.2%) patients had ever visited a rheumatologist. Axial SpA was diagnosed in 18 (27.3%) patients, peripheral SpA in 20 (30.3%) patients and another rheumatic disorder in 14 (21.2%) patients.
Conclusion: Musculoskeletal SpA features are frequently present in patients with IBD. However, a substantial group of patients is not evaluated by a rheumatologist. Gastroenterologists play a key role in early referral of this often debilitating disease.
HISTORIQUE :: Les symptômes musculosquelettiques qui appartiennent au spectre de la spondyloarthrite séronégative (SpA) sont les principales manifestations extra-intestinales chez les patients atteints d’une maladie inflammatoire de l’intestin (MII) et peuvent s’associer à un important fardeau de maladie. Les patients chez qui on craint une SpA devrait être aiguillés vers un rhumatologue pour subir une évaluation plus approfondie.
OBJECTIF :: Examiner la prévalence autodéclarée de caractéristiques musculosquelettiques de SpA dans une cohorte de patients atteints d’une MII et comparer les résultats avec le nombre d’aiguillages vers un rhumatologue.
MÉTHODOLOGIE :: Une infirmière de recherche formée a passé en entrevue des patients consécutifs atteints d’une MII afin de connaître leurs caractéristiques éventuelles de SpA au moyen d’un questionnaire standardisé sur la présence ou les antécédents de douleurs dorsales inflammatoires, d’arthrite périphérique, d’enthésite, de dactylite, de psoriasis, d’uvéite et de réponse aux anti-inflammatoires non stéroïdiens. Les chercheurs ont vérifié le dossier de tous les patients afin d’établir s’ils avaient déjà vu un rhumatologue et obtenu un diagnostic de problème rhumatismal.
RÉSULTATS :: Au total, 129 des 350 patients (36,9 %) ont déclaré au moins une caractéristique musculosquelettique de SpA. Il n’y avait pas de différence significative entre les patients atteints de la maladie de Crohn et de la colite ulcéreuse. L’examen des dossiers médicaux a révélé que 66 patients (51,2 %) n’avaient jamais consulté un rhumatologue. On avait diagnostiqué une SpA axiale chez 18 patients (27,3 %), une SpA périphérique chez 20 patients (30,3 %) et un autre trouble rhumatismal chez 14 patients (21,2 %).
CONCLUSION :: Les patients ayant une MII présentent souvent des caractéristiques musculosquelettiques de SpA. Cependant, un groupe important de patients n’est pas évalué par une rhumatologue. Les gastroentérologues ont un rôle essentiel à jouer pour l’aiguillage rapide des patients en vue de traiter cette maladie souvent débilitante.
Figures
Comment in
-
Multidisciplinary teams as standard of care in inflammatory bowel disease.Can J Gastroenterol. 2013 Apr;27(4):198. doi: 10.1155/2013/710671. Can J Gastroenterol. 2013. PMID: 23616956 Free PMC article. No abstract available.
References
-
- Greenstein AJ, Janowitz HD, Sachar DB. The extra-intestinal complications of Crohn’s disease and ulcerative colitis: A study of 700 patients. Medicine (Baltimore) 1976;55:401–12. - PubMed
-
- Moll JM, Haslock I, Macrae IF, Wright V. Associations between ankylosing spondylitis, psoriatic arthritis, Reiter’s disease, the intestinal arthropathies, and Behcet’s syndrome. Medicine (Baltimore) 1974:343–64. - PubMed
-
- Rudwaleit M. New approaches to diagnosis and classification of axial and peripheral spondyloarthritis. Curr Opin Rheumatol. 2010;22:375–80. - PubMed
-
- Ibn Yacoub Y, Amine B, Laatiris A, Bensabbah R, Hajjaj-Hassouni N. Relationship between diagnosis delay and disease features in Moroccan patients with ankylosing spondylitis. Rheumatol Int. 2012;32:357–60. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources