

Immunoglobulin G4-related disease mimicking asthma
- PMID: 23616963
- PMCID: PMC3630040
- DOI: 10.1155/2013/619453
Immunoglobulin G4-related disease mimicking asthma
Abstract
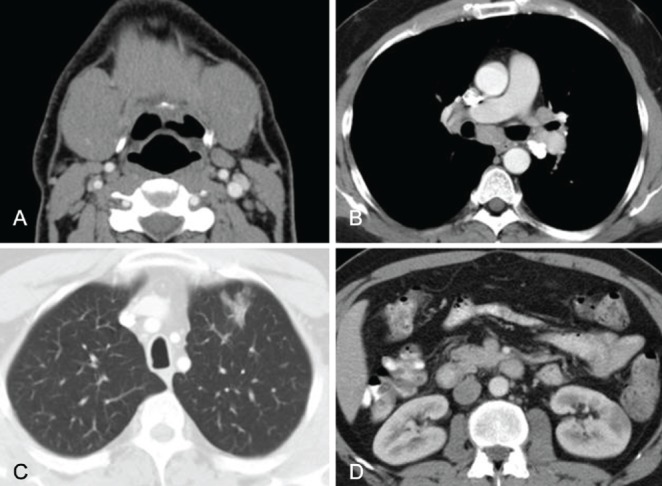
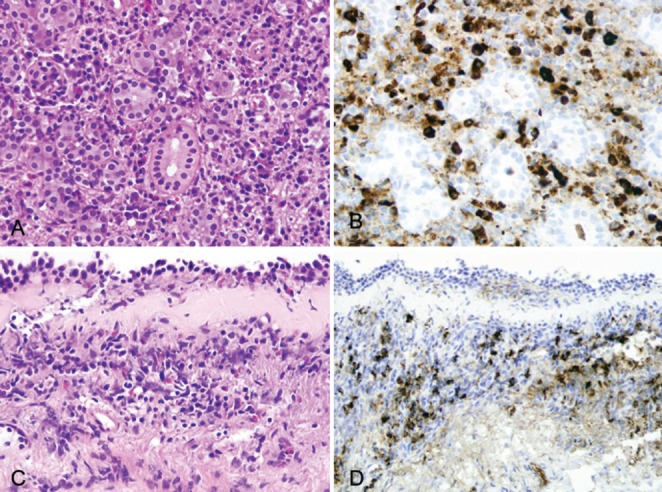
Immunoglobulin (Ig) G4-related disease (also known as 'IgG4-related sclerosing disease', 'IgG4-related systemic disease' or 'hyper-IgG4-disease') is a recently recognized systemic fibroinflammatory disease associated with IgG4-positive plasma cells in tissue lesions. IgG4-related disease was initially described as autoimmune pancreatitis, but it is now known to affect virtually any organ. The authors describe a patient presenting with multi-organ manifestations, including airway inflammation mimicking asthma, pulmonary parenchymal infiltrates, intrathoracic lymphadenopathy, submandibular gland swelling and a kidney mass.
La maladie liée aux immunoglobulines (Ig) G4 (aussi appelée maladie sclérosante liée aux IgG4 ou syndrome d’hyper-IgG4) est une maladie fibro-inflammatoire systémique récemment reconnue qui s’associe à des cellules plasmatiques positives aux IgG4 contenues dans les lésions tissulaires. La maladie liée aux IgG4 a d’abord été décrite comme une pancréatite auto-immune, mais on sait maintenant qu’elle peut toucher à peu près n’importe quel organe. Les auteurs décrivent le cas d’un patient atteint de manifestations multiorganiques, y compris une inflammation des voies aériennes imitant l’asthme, des infiltrats pulmonaires parenchymateux, une lymphadénopathie intrathoracique, un œdème des glandes sous-maxillaires et une masse rénale.
Figures
References
-
- Ryu JH, Sekiguchi H, Yi ES. Pulmonary manifestations of immunoglobulin G4-related sclerosing disease. Eur Respir J. 2012;39:180–6. - PubMed
-
- Khosroshahi A, Stone JH. A clinical overview of IgG4-related systemic disease. Curr Opin Rheumatol. 2011;23:57–66. - PubMed
-
- Khosroshahi A, Deshpande V, Stone JH. The clinical and pathological features of IgG(4)-related disease. Curr Rheumatol Rep. 2011;13:473–81. - PubMed
-
- Zen Y, Nakanuma Y. IgG4-related disease: A cross-sectional study of 114 cases. Am J Surg Pathol. 2010;34:1812–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
