

Neonatal clinical pharmacology
- PMID: 23617305
- PMCID: PMC3758438
- DOI: 10.1111/pan.12176
Neonatal clinical pharmacology
Abstract
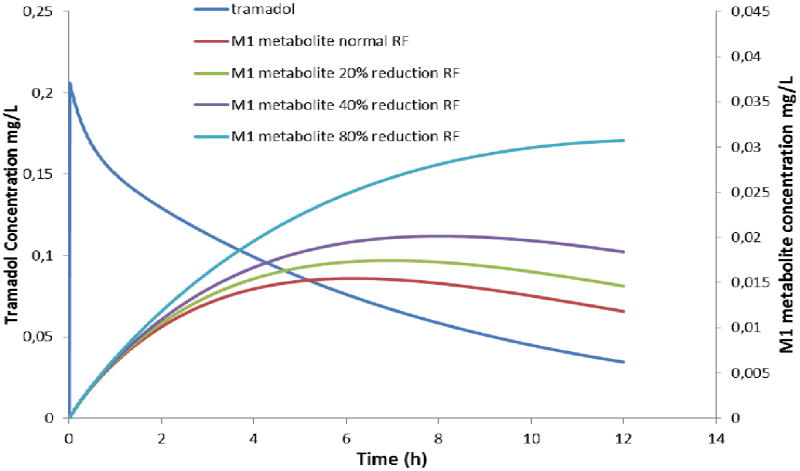
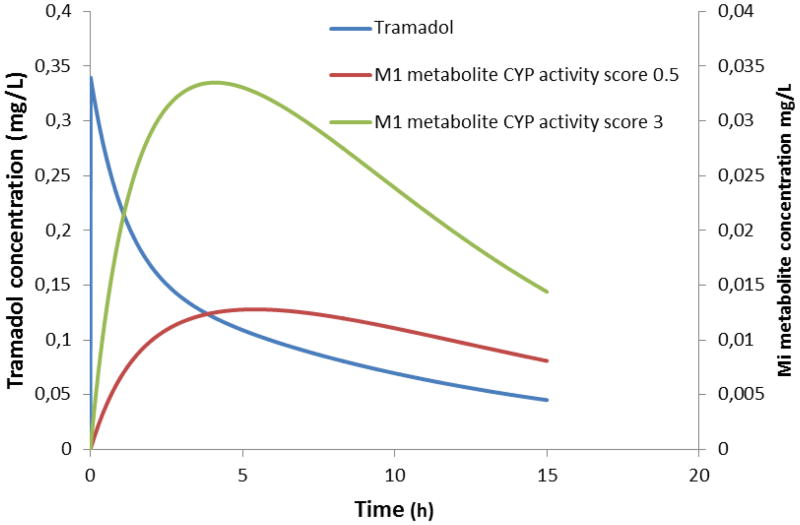
Effective and safe drug administration in neonates should be based on integrated knowledge on the evolving physiological characteristics of the infant who will receive the drug and the pharmacokinetics (PK) and pharmacodynamics (PD) of a given drug. Consequently, clinical pharmacology in neonates is as dynamic and diverse as the neonates we admit to our units while covariates explaining the variability are at least as relevant as median estimates. The unique setting of neonatal clinical pharmacology will be highlighted based on the hazards of simple extrapolation of maturational drug clearance when only based on 'adult' metabolism (propofol, paracetamol). Second, maturational trends are not at the same pace for all maturational processes. This will be illustrated based on the differences between hepatic and renal maturation (tramadol, morphine, midazolam). Finally, pharmacogenetics should be tailored to neonates, not just mirror adult concepts. Because of this diversity, clinical research in the field of neonatal clinical pharmacology is urgently needed and facilitated through PK/PD modeling. In addition, irrespective of already available data to guide pharmacotherapy, pharmacovigilance is needed to recognize specific side effects. Consequently, pediatric anesthesiologists should consider to contribute to improved pharmacotherapy through clinical trial design and collaboration, as well as reporting on adverse effects of specific drugs.
Keywords: anesthesia; infant; newborn; ontogeny; pharmacodynamics; pharmacokinetics.
© 2013 John Wiley & Sons Ltd.
Figures
References
-
- Anderson BJ, Allegaert K. The pharmacology of anaesthetics in the neonate. Best Pract Res Clin Anaesthesiol. 2010;24:419–431. - PubMed
-
- Smits A, Kulo A, de Hoon JN, Allegaert K. Pharmacokinetics of drugs in neonates: pattern recognition beyond compound specific observations. Curr Pharm Des. 2012;18:3119–3146. - PubMed
-
- Anderson BJ. Pharmacology in the very young: anaesthetic implications. Eur J Anaesthesiol. 2012;29:261–270. - PubMed
-
- Sumpter A, Anderson BJ. Pediatric pharmacology in the first year of life. Curr Opin Anaesthesiol. 2009;22:469–475. - PubMed
-
- Allegaert K, Verbesselt R, Naulaers G, et al. Developmental pharmacology: neonates are not just small adults. Acta Clin Belg. 2008;63:16–24. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
