

Persistent nasal methicillin-resistant staphylococcus aureus carriage in hemodialysis outpatients: a predictor of worse outcome
- PMID: 23617360
- PMCID: PMC3651301
- DOI: 10.1186/1471-2369-14-93
Persistent nasal methicillin-resistant staphylococcus aureus carriage in hemodialysis outpatients: a predictor of worse outcome
Abstract
Background: Nasal colonization with methicillin-resistant Staphylococcus aureus (MRSA) is a well defined risk factor for subsequent bacteremia and death in various groups of patients, but its impact on outcome in patients receiving long-term hemodialysis (HD) is under debate.
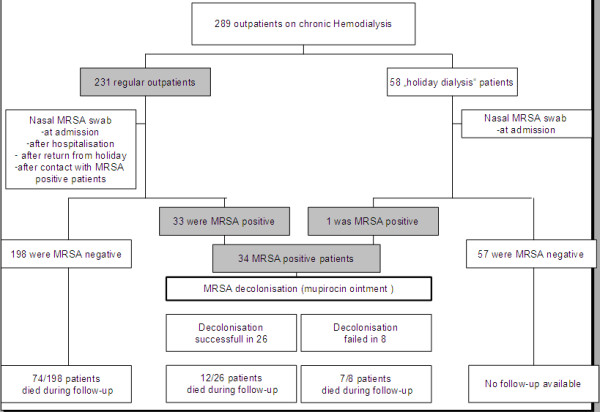
Methods: This prospective interventional cohort study (performed 2004 to 2010) enrolled 289 HD outpatients of an urban dialysis-unit. Nasal swab cultures for MRSA were performed in all patients upon first admission, at transfer from another dialysis facility or readmission after hospitalisation. Nasal MRSA carriers were treated in a separate ward and received mupirocin nasal ointment. Concomitant extra-nasal MRSA colonization was treated with 0.2% chlorhexidine mouth rinse (throat) or octenidine dihydrochloride containing antiseptic soaps and 2% chlorhexidine body washes (skin). Clinical data and outcome of carriers and noncarriers were systematically analyzed.
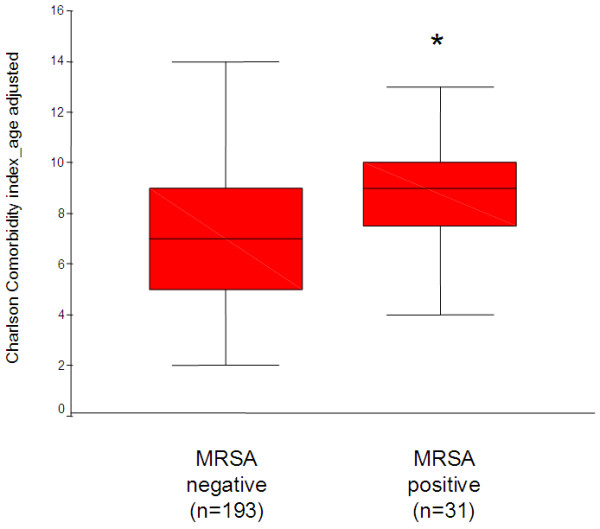
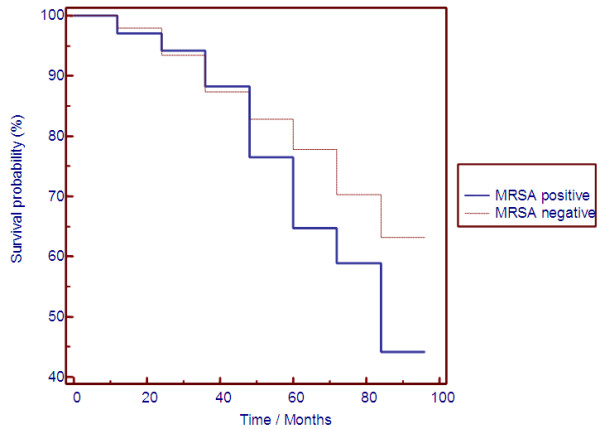
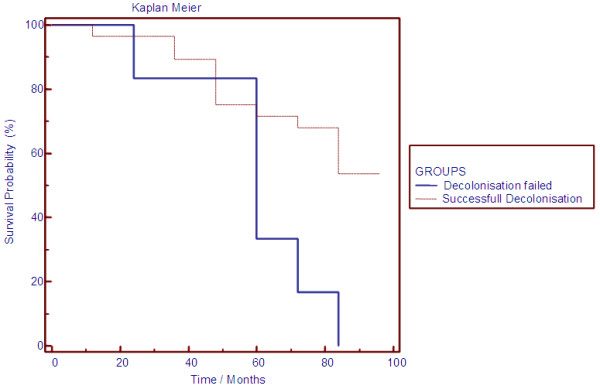
Results: The screening approach identified 34 nasal MRSA carriers (11.7%). Extra-nasal MRSA colonization was observed in 11/34 (32%) nasal MRSA carriers. History of malignancy and an increased Charlson Comorbidity Index were significant predictors for nasal MRSA carriers, whereas traditional risk factors for MRSA colonization or markers of inflammation or malnutrition were not able to discriminate. Kaplan-Meier analysis demonstrated significant survival differences between MRSA carriers and noncarriers. Mupirocin ointment persistently eliminated nasal MRSA colonization in 26/34 (73.5%) patients. Persistent nasal MRSA carriers with failure of this eradication approach had an extremely poor prognosis with an all-cause mortality rate >85%.
Conclusions: Nasal MRSA carriage with failure of mupirocin decolonization was associated with increased mortality despite a lack of overt clinical signs of infection. Further studies are needed to demonstrate whether nasal MRSA colonization represents a novel predictor of worse outcome or just another surrogate marker of the burden of comorbid diseases leading to fatal outcome in HD patients.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
