

Metabolic dysfunction in pulmonary hypertension: the expanding relevance of the Warburg effect
- PMID: 23617881
- PMCID: PMC3736346
- DOI: 10.1111/eci.12104
Metabolic dysfunction in pulmonary hypertension: the expanding relevance of the Warburg effect
Abstract
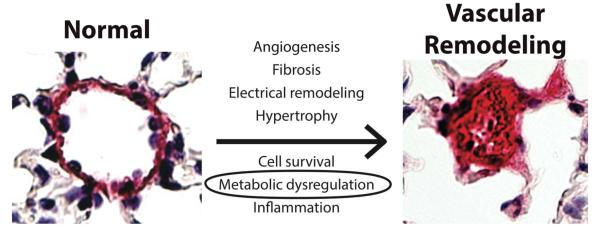
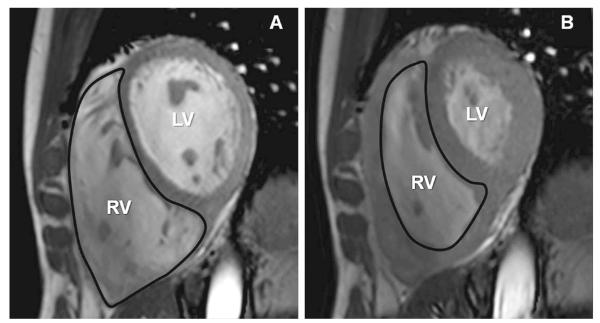
Background: Pulmonary hypertension (PH) is an enigmatic vascular syndrome characterized by increased pulmonary arterial pressure and adverse remodelling of the pulmonary arterioles and often of the right ventricle. Drawing parallels with tumourigenesis, recent endeavours have explored the relationship between metabolic dysregulation and PH pathogenesis.
Design: We will discuss the general mechanisms by which cellular stressors such as hypoxia and inflammation alter cellular metabolism. Based on those principles, we will explore the development of a corresponding metabolic pathophenotype in PH, with a focus on WHO Groups I and III, and the implications that these alterations may have for future treatment of this disease.
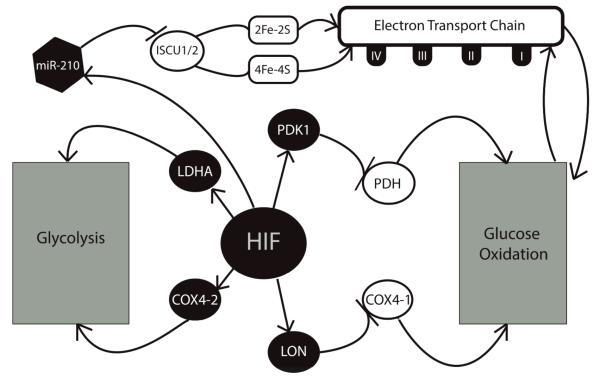
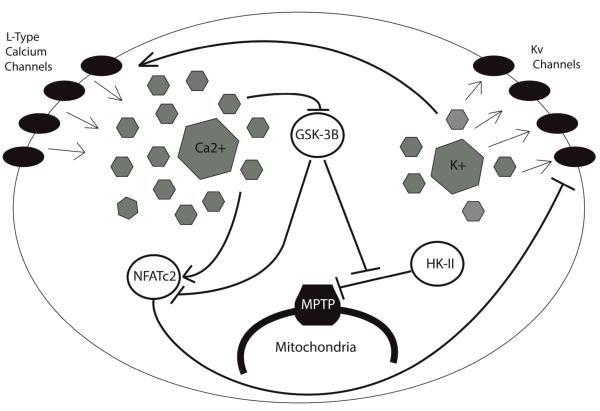
Results: Investigation of metabolic dysregulation in both the pulmonary vasculature and right ventricle during PH pathogenesis has provided a more unifying understanding of how disparate disease triggers coordinate end-stage disease manifestations. Namely, as defined originally in various cancers, the Warburg effect describes a chronic shift in energy production from mitochondrial oxidative phosphorylation to glycolysis. In many cases, this Warburg phenotype may serve as a central causative mechanism for PH progression, largely driving cellular hyperproliferation and resistance to apoptosis. Consequently, new therapeutic strategies have been increasingly pursued that target the Warburg phenotype. Finally, new technologies are increasingly becoming available to probe more completely the complexities of metabolic cellular reprogramming and may reveal distinct metabolic pathways beyond the Warburg effect that drive PH.
Conclusion: Studies of metabolic dysregulation in PH are just emerging but may offer powerful therapeutic means to prevent or even reverse disease progression at the molecular level.
Keywords: Glycolysis; Warburg effect; hypoxia; metabolism; mitochondria; pulmonary hypertension.
© 2013 Stichting European Society for Clinical Investigation Journal Foundation. Published by John Wiley & Sons Ltd.
Figures
References
-
- McLaughlin VV, Archer SL, Badesch DB, Barst RJ, Farber HW, Lindner JR, Mathier MA, McGoon MD, Park MH, Rosenson RS, Rubin LJ, Tapson VF, Varga J, Harrington RA, Anderson JL, Bates ER, Bridges CR, Eisenberg MJ, Ferrari VA, Grines CL, Hlatky MA, Jacobs AK, Kaul S, Lichtenberg RC, Moliterno DJ, Mukherjee D, Pohost GM, Schofield RS, Shubrooks SJ, Stein JH, Tracy CM, Weitz HH, Wesley DJ. Accf/aha, accf/aha 2009 expert consensus document on pulmonary hypertension: A report of the american college of cardiology foundation task force on expert consensus documents and the american heart association: Developed in collaboration with the american college of chest physicians, american thoracic society, inc., and the pulmonary hypertension association. Circulation. 2009;119:2250–2294. - PubMed
-
- Simonneau G, Robbins IM, Beghetti M, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2009;54:S43–S54. - PubMed
-
- Barberà JA, Peinado VI, Santos S. Pulmonary hypertension in chronic obstructive pulmonary disease. Eur Respir J. 2003;21:892–905. - PubMed
-
- Lourenço AP, Fontoura D, Henriques-Coelho T, Leite-Moreira AF. Current pathophysiological concepts and management of pulmonary hypertension. Int J Cardiol. 2012;155:350–361. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
