

Implementation of misoprostol for postabortion care in Kenya and Uganda: a qualitative evaluation
- PMID: 23618341
- PMCID: PMC3636418
- DOI: 10.3402/gha.v6i0.19649
Implementation of misoprostol for postabortion care in Kenya and Uganda: a qualitative evaluation
Abstract
Objective: Evaluate implementation of misoprostol for postabortion care (MPAC) in two African countries.
Design: Qualitative, program evaluation.
Setting: Twenty-five public and private health facilities in Rift Valley Province, Kenya, and Kampala Province, Uganda.
Sample: Forty-five MPAC providers, health facility managers, Ministry of Health officials, and non-governmental (NGO) staff involved in program implementation.
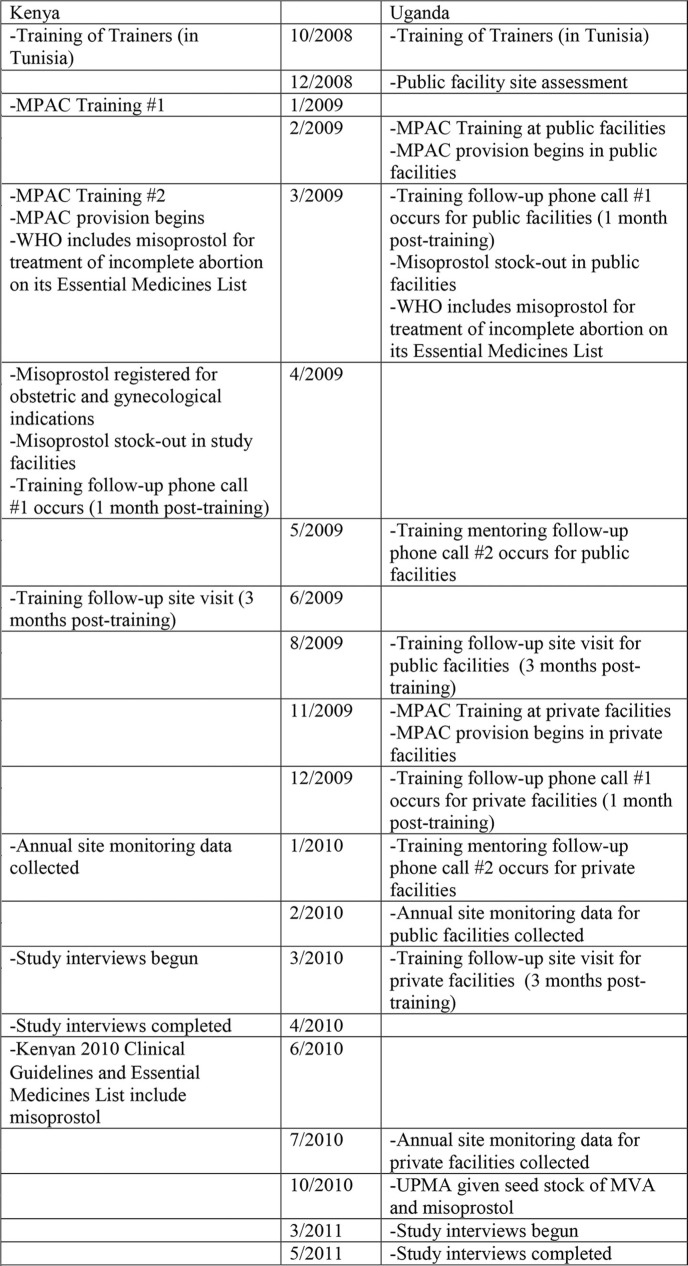
Methods and main outcome measures: In both countries, the Ministry of Health, local health centers and hospitals, and NGO staff developed evidence-based service delivery protocols to introduce MPAC in selected facilities; implementation extended from January 2009 to October 2010. Semi-structured, in-depth interviews evaluated the implementation process, identified supportive and inhibitive policies for implementation, elicited lessons learned during the process, and assessed provider satisfaction and providers' impressions of client satisfaction with MPAC. Project reports were also reviewed.
Results: In both countries, MPAC was easy to use, and freed up provider time and health facility resources traditionally necessary for provision of PAC with uterine aspiration. On-going support of providers following training ensured high quality of care. Providers perceived that many women preferred MPAC, as they avoided instrumentation of the uterus, hospital admission, cost, and stigma associated with abortion. Appropriate registration of misoprostol for use in the pilot, and maintaining supplies of misoprostol, were significant challenges to service provision. Support from the Ministry of Health was necessary for successful implementation; lack of country-based standards and guidelines for MPAC created challenges.
Conclusions: MPAC is simple, cost-effective and can be readily implemented in settings with high rates of abortion-related mortality.
Keywords: implementation research; misoprostol; postabortion care.
Figures
Comment in
-
Osur et al.'s Implementation of misoprostol for postabortion care in Kenya and Uganda: a qualitative evaluation.Glob Health Action. 2012 Jul 18;6:21786. doi: 10.3402/gha.v6i0.21786. Glob Health Action. 2012. PMID: 23870184 Free PMC article. No abstract available.
-
Letter to the editor.Glob Health Action. 2013 Jul 18;6:21787. doi: 10.3402/gha.v6i0.21787. Glob Health Action. 2013. PMID: 23870185 Free PMC article. No abstract available.
References
-
- Grimes DA. Unsafe abortion: the silent scourge. Br Med Bull. 2003;67:99–113. - PubMed
-
- Singh S, Wulf D, Hussain R, Bankole A, Sedgh G. Abortion worldwide: a decade of uneven progress. New York: Guttmacher Institute; 2009.
-
- Sedgh G, Singh S, Shah I, Ahman E, Henshaw S, Bankole A. Induced abortion: incidence and trends worldwide from 1995 to 2008. Lancet. 2012;379:625–32. - PubMed
-
- Kenya Penal Code. 1973. Sections 158–160, 214 and 240. Kenya.
-
- Constitution of the Republic of Uganda. Uganda; 1995. Part XIV(b), XX, articles 22.2, 27, 34(3) and 41.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources