

KRAS mutations are associated with solid growth pattern and tumor-infiltrating leukocytes in lung adenocarcinoma
- PMID: 23619604
- PMCID: PMC3732528
- DOI: 10.1038/modpathol.2013.74
KRAS mutations are associated with solid growth pattern and tumor-infiltrating leukocytes in lung adenocarcinoma
Abstract
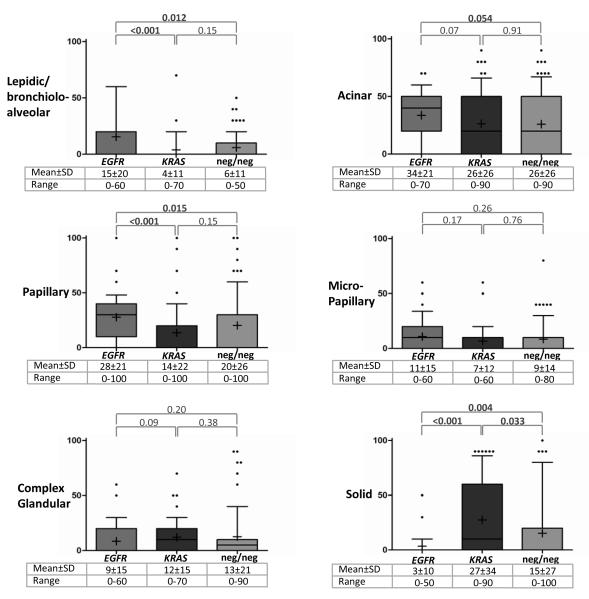
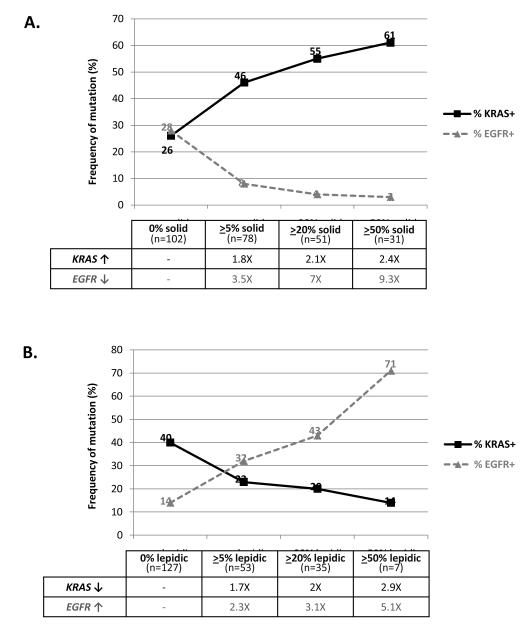
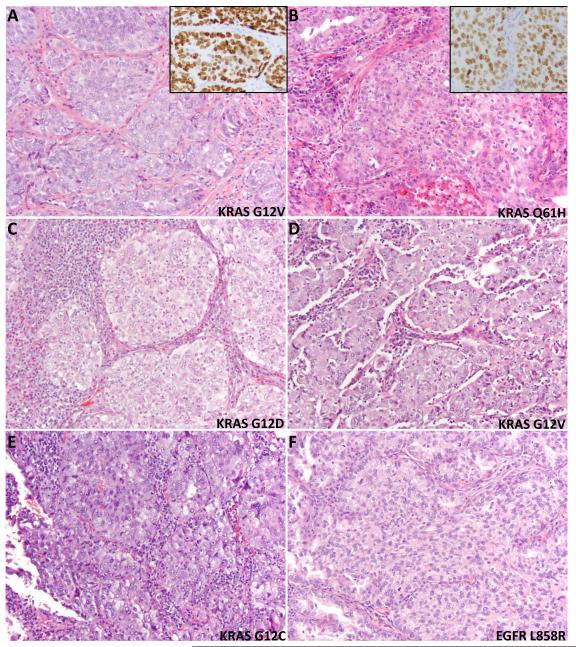
KRAS mutations define a clinically distinct subgroup of lung adenocarcinoma patients, characterized by smoking history, resistance to EGFR-targeted therapies, and adverse prognosis. Whether KRAS-mutated lung adenocarcinomas also have distinct histopathological features is not well established. We tested 180 resected lung adenocarcinomas for KRAS and EGFR mutations by high-sensitivity mass spectrometry-based genotyping (Sequenom) and PCR-based sizing assays. All tumors were assessed for the proportion of standard histological patterns (lepidic, acinar, papillary, micropapillary, solid, and mucinous), several other histological and clinical parameters, and TTF-1 expression by immunohistochemistry. Among 180 carcinomas, 63 (35%) had KRAS mutations (KRAS+), 35 (19%) had EGFR mutations (EGFR+), and 82 (46%) had neither mutation (KRAS-/EGFR-). Solid growth pattern was significantly over-represented in KRAS+ carcinomas: the mean±s.d. for the amount of solid pattern in KRAS+ carcinomas was 27±34% compared with 3±10% in EGFR+ (P<0.001) and 15±27% in KRAS-/EGFR- (P=0.033) tumors. Furthermore, at least focal (≥20%) solid component was more common in KRAS+ (28/63; 44%) compared with EGFR+ (2/35; 6%; P<0.001) and KRAS-/EGFR- (21/82; 26%; P=0.022) carcinomas. KRAS mutations were also over-represented in mucinous carcinomas and were significantly associated with the presence of tumor-infiltrating leukocytes and heavier smoking history. EGFR mutations were associated with non-mucinous non-solid patterns, particularly lepidic and papillary, lack of necrosis, lack of cytological atypia, hobnail cytology, TTF-1 expression, and never/light smoking history. In conclusion, extended molecular and clinicopathological analysis of lung adenocarcinomas reveals a novel association of KRAS mutations with solid histology and tumor-infiltrating inflammatory cells and expands on several previously recognized morphological and clinical associations of KRAS and EGFR mutations. Solid growth pattern was recently shown to be a strong predictor of aggressive behavior in lung adenocarcinomas, which may underlie the unfavorable prognosis associated with KRAS mutations in these tumors.
Figures
References
-
- Malumbres M, Barbacid M. RAS oncogenes: the first 30 years. Nat Rev Cancer. 2003;3:459–65. - PubMed
-
- Bos JL. ras oncogenes in human cancer: a review. Cancer Res. 1989;49:4682–9. - PubMed
-
- Santos E, Martin-Zanca D, Reddy EP, et al. Malignant activation of a K-ras oncogene in lung carcinoma but not in normal tissue of the same patient. Science. 1984;223:661–4. - PubMed
-
- Riely GJ, Marks J, Pao W. KRAS mutations in non-small cell lung cancer. Proc Am Thorac Soc. 2009;6:201–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
