

COPD surveillance--United States, 1999-2011
- PMID: 23619732
- PMCID: PMC3707177
- DOI: 10.1378/chest.13-0809
COPD surveillance--United States, 1999-2011
Abstract
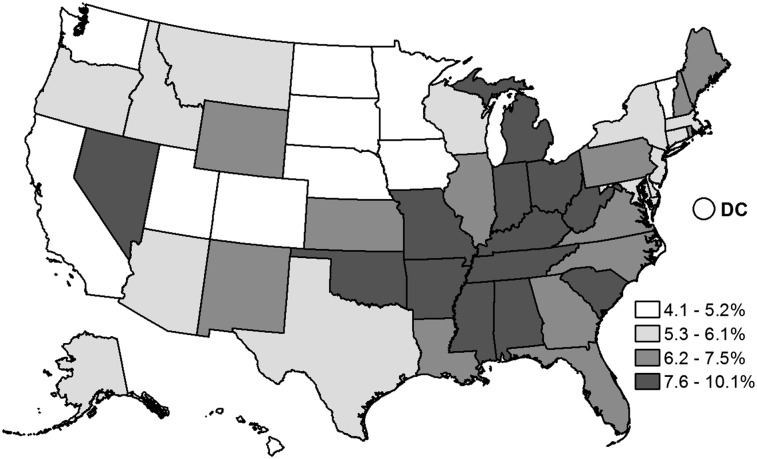
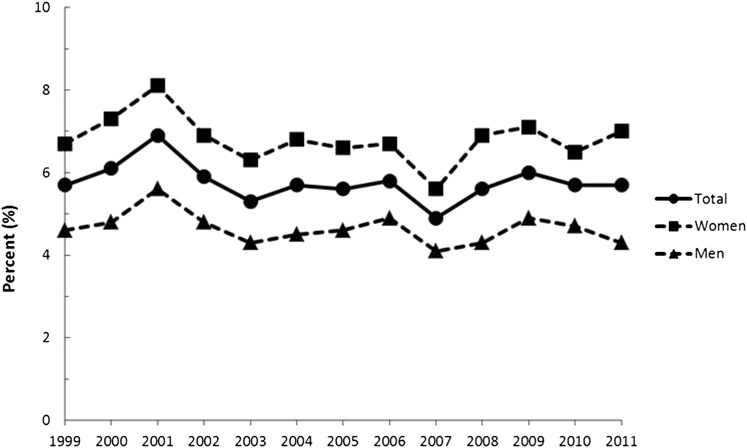
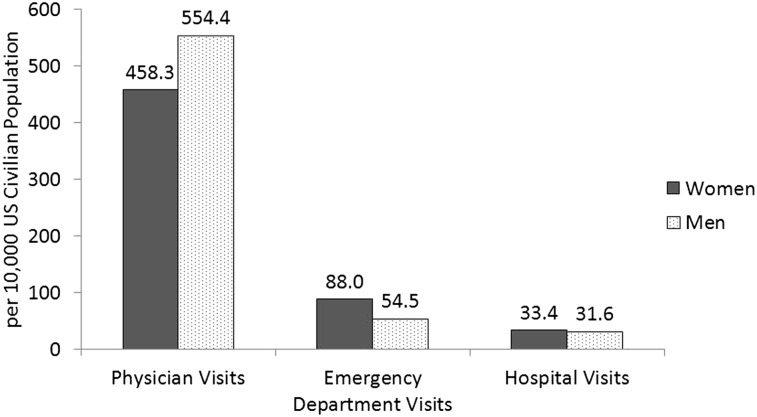
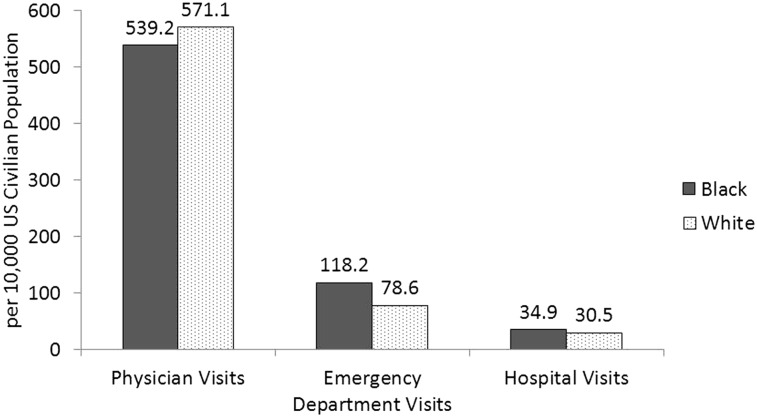
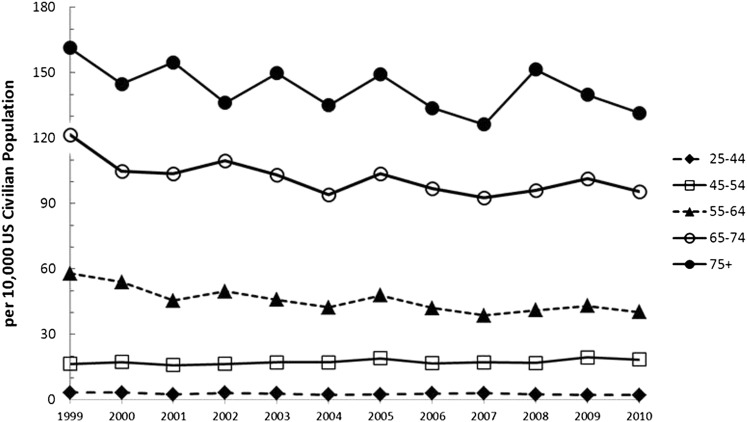
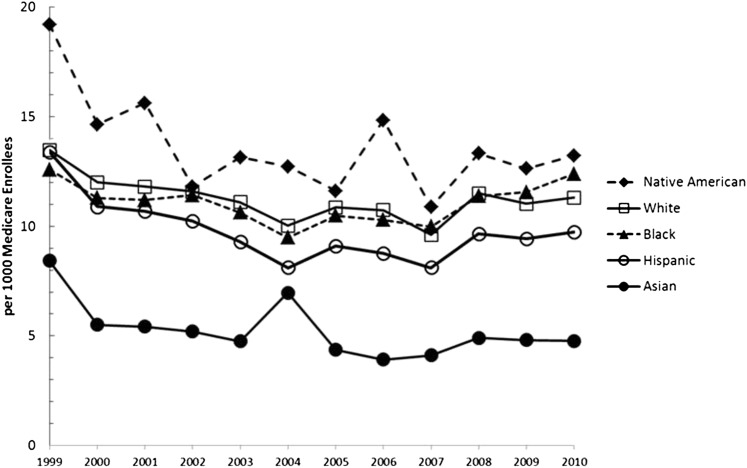
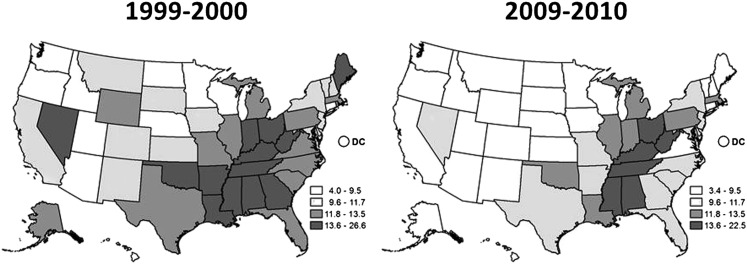
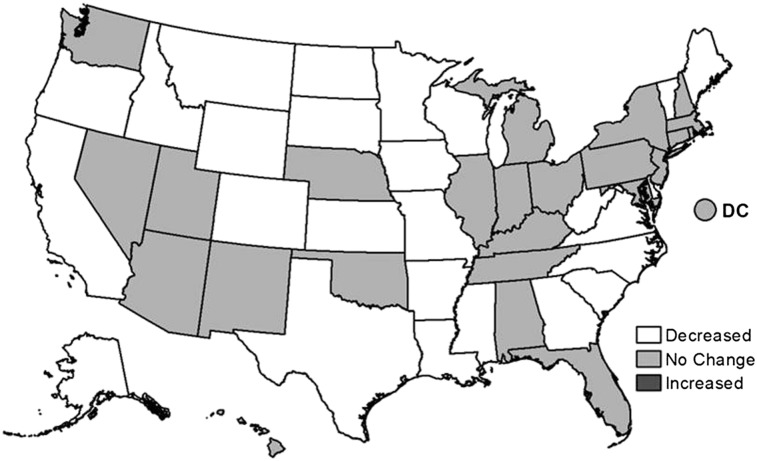
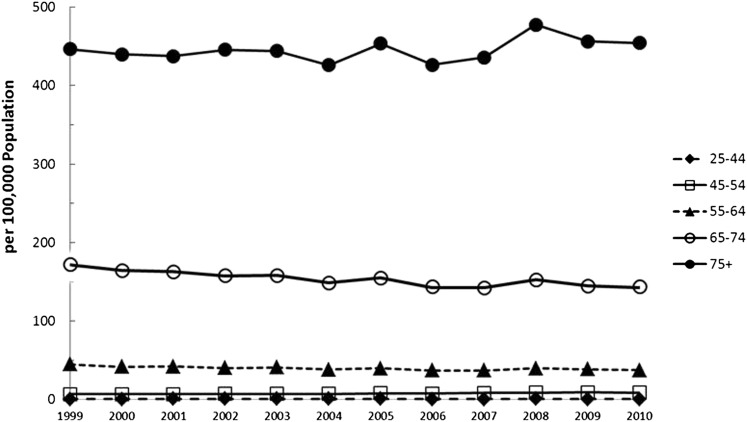
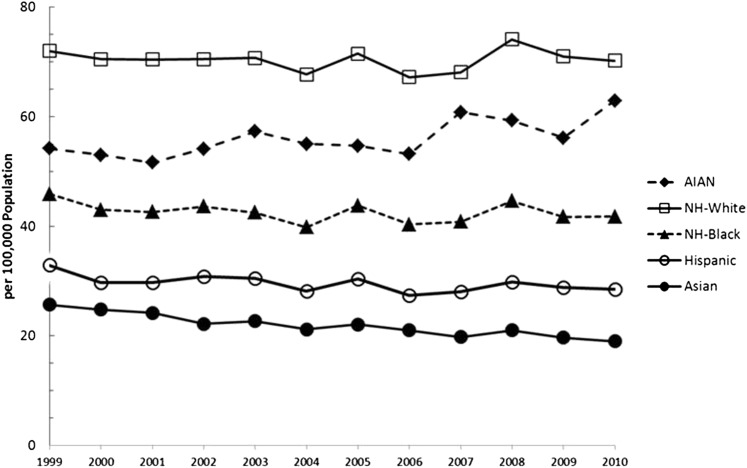
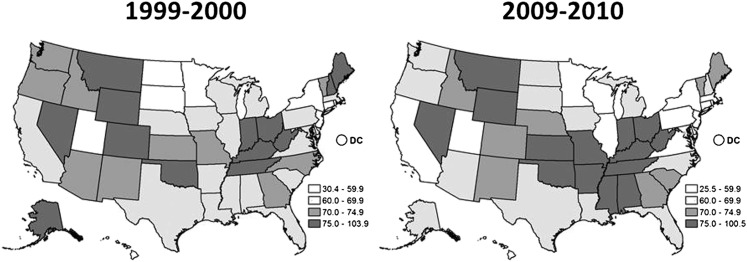
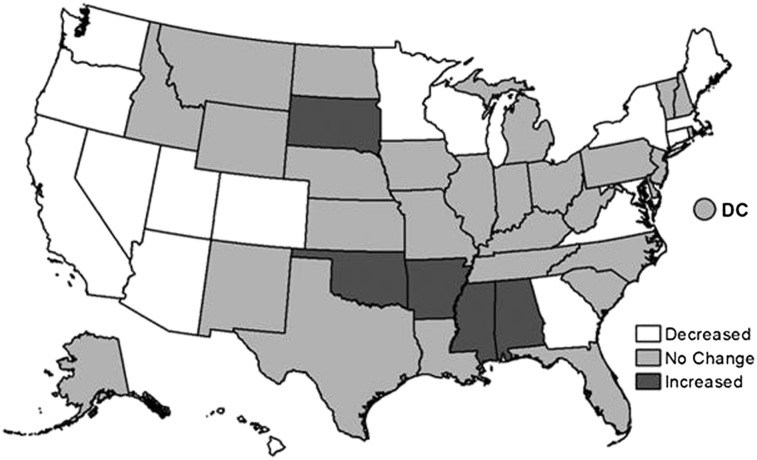
This report updates surveillance results for COPD in the United States. For 1999 to 2011, data from national data systems for adults aged≥25 years were analyzed. In 2011, 6.5% of adults (approximately 13.7 million) reported having been diagnosed with COPD. From 1999 to 2011, the overall age-adjusted prevalence of having been diagnosed with COPD declined (P=.019). In 2010, there were 10.3 million (494.8 per 10,000) physician office visits, 1.5 million (72.0 per 10,000) ED visits, and 699,000 (32.2 per 10,000) hospital discharges for COPD. From 1999 to 2010, no significant overall trends were noted for physician office visits and ED visits; however, the age-adjusted hospital discharge rate for COPD declined significantly (P=.001). In 2010 there were 312,654 (11.2 per 1,000) Medicare hospital discharge claims submitted for COPD. Medicare claims (1999-2010) declined overall (P=.045), among men (P=.022) and among enrollees aged 65 to 74 years (P=.033). There were 133,575 deaths (63.1 per 100,000) from COPD in 2010. The overall age-adjusted death rate for COPD did not change during 1999 to 2010 (P=.163). Death rates (1999-2010) increased among adults aged 45 to 54 years (P<.001) and among American Indian/Alaska Natives (P=.008) but declined among those aged 55 to 64 years (P=.002) and 65 to 74 years (P<.001), Hispanics (P=.038), Asian/Pacific Islanders (P<.001), and men (P=.001). Geographic clustering of prevalence, Medicare hospitalizations, and deaths were observed. Declines in the age-adjusted prevalence, death rate in men, and hospitalizations for COPD since 1999 suggest progress in the prevention of COPD in the United States.
Figures
References
-
- Miniño AM, Xu J, Kochanek KD, Division of Vital Statistics.Deaths: preliminary data for 2008. Natl Vital Stat Rep. 2010;59(2):1-52. - PubMed
-
- Centers for Disease Control and Prevention (CDC) Smoking-attributable mortality, years of potential life lost, and productivity losses—United States, 2000-2004. MMWR Morb Mortal Wkly Rep. 2008;57(45):1226-1228 - PubMed
-
- Engström CP, Persson LO, Larsson S, Sullivan M. Health-related quality of life in COPD: why both disease-specific and generic measures should be used. Eur Respir J. 2001;18(1):69-76 - PubMed
-
- Viegi G, Pistelli F, Sherrill DL, Maio S, Baldacci S, Carrozzi L. Definition, epidemiology and natural history of COPD. Eur Respir J. 2007;30(5):993-1013 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
