

New MR imaging assessment tool to define brain abnormalities in very preterm infants at term
- PMID: 23620070
- PMCID: PMC4163698
- DOI: 10.3174/ajnr.A3521
New MR imaging assessment tool to define brain abnormalities in very preterm infants at term
Abstract
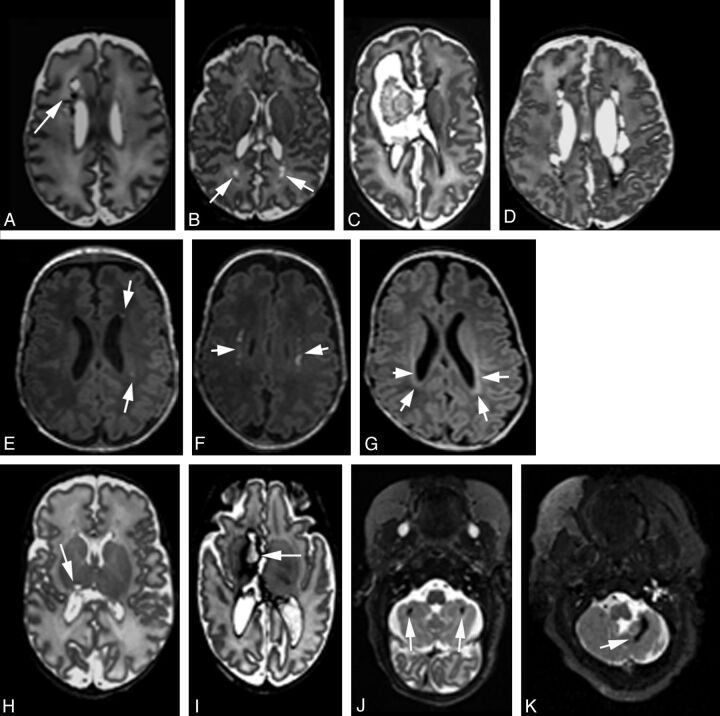
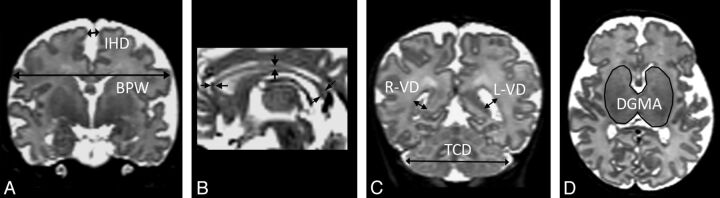
Background and purpose: WM injury is the dominant form of injury in preterm infants. However, other cerebral structures, including the deep gray matter and the cerebellum, can also be affected by injury and/or impaired growth. Current MR imaging injury assessment scales are subjective and are challenging to apply. Thus, we developed a new assessment tool and applied it to MR imaging studies obtained from very preterm infants at term age.
Materials and methods: MR imaging scans from 97 very preterm infants (< 30 weeks' gestation) and 22 healthy term-born infants were evaluated retrospectively. The severity of brain injury (defined by signal abnormalities) and impaired brain growth (defined with biometrics) was scored in the WM, cortical gray matter, deep gray matter, and cerebellum. Perinatal variables for clinical risks were collected.
Results: In very preterm infants, brain injury was observed in the WM (n=23), deep GM (n=5), and cerebellum (n=23). Combining measures of injury and impaired growth showed moderate to severe abnormalities most commonly in the WM (n=38) and cerebellum (n=32) but still notable in the cortical gray matter (n=16) and deep gray matter (n=11). WM signal abnormalities were associated with a reduced deep gray matter area but not with cerebellar abnormality. Intraventricular and/or parenchymal hemorrhage was associated with cerebellar signal abnormality and volume reduction. Multiple clinical risk factors, including prolonged intubation, prolonged parenteral nutrition, postnatal corticosteroid use, and postnatal sepsis, were associated with increased global abnormality on MR imaging.
Conclusions: Very preterm infants demonstrate a high prevalence of injury and growth impairment in both the WM and gray matter. This MR imaging scoring system provides a more comprehensive and objective classification of the nature and extent of abnormalities than existing measures.
Figures
Similar articles
-
Validation of an MRI Brain Injury and Growth Scoring System in Very Preterm Infants Scanned at 29- to 35-Week Postmenstrual Age.AJNR Am J Neuroradiol. 2017 Jul;38(7):1435-1442. doi: 10.3174/ajnr.A5191. Epub 2017 May 18. AJNR Am J Neuroradiol. 2017. PMID: 28522659 Free PMC article.
-
T2 at MR imaging is an objective quantitative measure of cerebral white matter signal intensity abnormality in preterm infants at term-equivalent age.Radiology. 2009 Jul;252(1):209-17. doi: 10.1148/radiol.2522080589. Radiology. 2009. PMID: 19561257
-
Defining the nature of the cerebral abnormalities in the premature infant: a qualitative magnetic resonance imaging study.J Pediatr. 2003 Aug;143(2):171-9. doi: 10.1067/S0022-3476(03)00357-3. J Pediatr. 2003. PMID: 12970628
-
Diffusion magnetic resonance imaging in preterm brain injury.Neuroradiology. 2013 Sep;55 Suppl 2:65-95. doi: 10.1007/s00234-013-1242-x. Epub 2013 Aug 14. Neuroradiology. 2013. PMID: 23942765 Review.
-
Neuroimaging of white matter injury, intraventricular and cerebellar hemorrhage.Clin Perinatol. 2014 Mar;41(1):69-82. doi: 10.1016/j.clp.2013.09.005. Epub 2013 Dec 17. Clin Perinatol. 2014. PMID: 24524447 Review.
Cited by
-
Endogenous erythropoietin concentrations and association with retinopathy of prematurity and brain injury in preterm infants.PLoS One. 2021 Jun 2;16(6):e0252655. doi: 10.1371/journal.pone.0252655. eCollection 2021. PLoS One. 2021. PMID: 34077474 Free PMC article.
-
Experience of early-life pain in premature infants is associated with atypical cerebellar development and later neurodevelopmental deficits.BMC Med. 2023 Nov 14;21(1):435. doi: 10.1186/s12916-023-03141-w. BMC Med. 2023. PMID: 37957651 Free PMC article.
-
Severity of prematurity and age impact early postnatal development of GABA and glutamate systems.Cereb Cortex. 2023 Jun 8;33(12):7386-7394. doi: 10.1093/cercor/bhad046. Cereb Cortex. 2023. PMID: 36843135 Free PMC article.
-
Structural connectivity at term equivalent age and language in preterm children at 2 years corrected.Brain Commun. 2024 Apr 10;6(2):fcae126. doi: 10.1093/braincomms/fcae126. eCollection 2024. Brain Commun. 2024. PMID: 38665963 Free PMC article.
-
Prevention of Neurological Sequelae in Preterm Infants.Brain Sci. 2023 May 2;13(5):753. doi: 10.3390/brainsci13050753. Brain Sci. 2023. PMID: 37239225 Free PMC article.
References
-
- Platt MJ, Cans C, Johnson A, et al. . Trends in cerebral palsy among infants of very low birthweight (<1500 g) or born prematurely (<32 weeks) in 16 European centres: a database study. Lancet 2007;369:43–50 - PubMed
-
- Robertson CM, Watt MJ, Yasui Y. Changes in the prevalence of cerebral palsy for children born very prematurely within a population-based program over 30 years. JAMA 2007;297:2733–40 - PubMed
-
- Anderson P, Doyle LW. Neurobehavioral outcomes of school-age children born extremely low birth weight or very preterm in the 1990s. JAMA 2003;289:3264–72 - PubMed
-
- Hack M, Flannery DJ, Schluchter M, et al. . Outcomes in young adulthood for very-low-birth-weight infants. N Engl J Med 2002;346:149–57 - PubMed
-
- Volpe JJ, Kinney HC, Jensen FE, et al. . Reprint of “The developing oligodendrocyte: key cellular target in brain injury in the premature infant”. Int J Dev Neurosci 2011;29:565–82 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical