

Intramedullary spinal cord metastases: MRI and relevant clinical features from a 13-year institutional case series
- PMID: 23620071
- PMCID: PMC7965414
- DOI: 10.3174/ajnr.A3526
Intramedullary spinal cord metastases: MRI and relevant clinical features from a 13-year institutional case series
Abstract
Background and purpose: Because intramedullary spinal cord metastasis is often a difficult diagnosis to make, our purpose was to perform a systematic review of the MR imaging and relevant baseline clinical features of intramedullary spinal cord metastases in a large series.
Materials and methods: Consecutive patients with intramedullary spinal cord metastasis with available pretreatment digital MR imaging examinations were identified. The MR imaging examination(s) for each patient was reviewed by 2 neuroradiologists for various imaging characteristics. Relevant clinical data were obtained.
Results: Forty-nine patients had 70 intramedullary spinal cord metastases, with 10 (20%) having multiple intramedullary spinal cord metastases; 8% (4/49) were asymptomatic. Primary tumor diagnosis was preceded by intramedullary spinal cord metastasis presentation in 20% (10/49) and by intramedullary spinal cord metastasis diagnosis in 10% (5/49); 98% (63/64) of intramedullary spinal cord metastases enhanced. Cord edema was extensive: mean, 4.5 segments, 3.6-fold larger than enhancing lesion, and ≥3 segments in 54% (37/69). Intratumoral cystic change was seen in 3% (2/70) and hemorrhage in 1% (1/70); 59% (29/49) of reference MR imaging examinations displayed other CNS or spinal (non-spinal cord) metastases, and 59% (29/49) exhibited the primary tumor/non-CNS metastases, with 88% (43/49) displaying ≥1 finding and 31% (15/49) displaying both findings. Patients with solitary intramedullary spinal cord metastasis were less likely than those with multiple intramedullary spinal cord metastases to have other CNS or spinal (non-spinal cord) metastases on the reference MR imaging (20/39 [51%] versus 9/10 [90%], respectively; P = .0263).
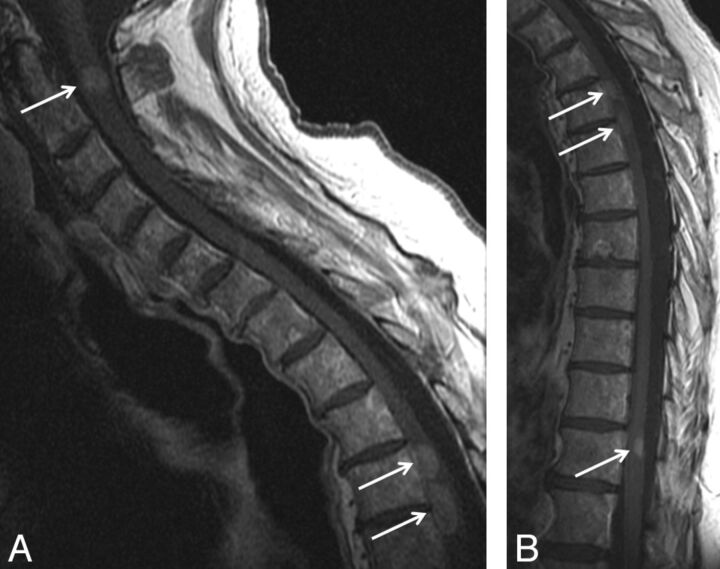
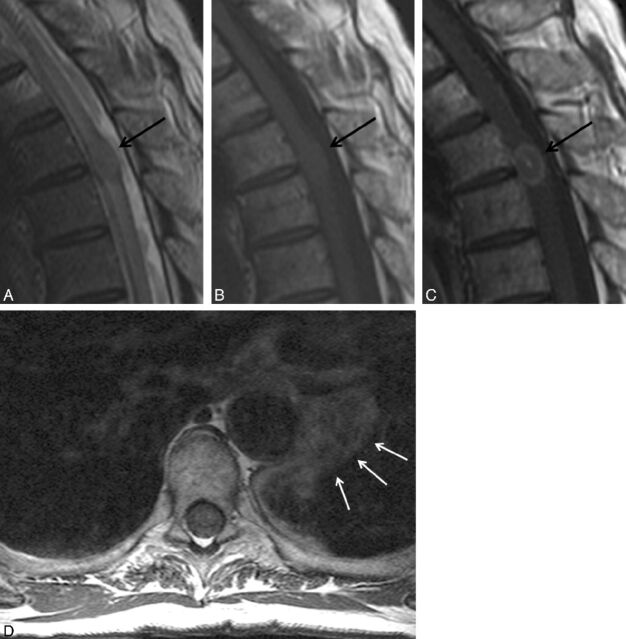
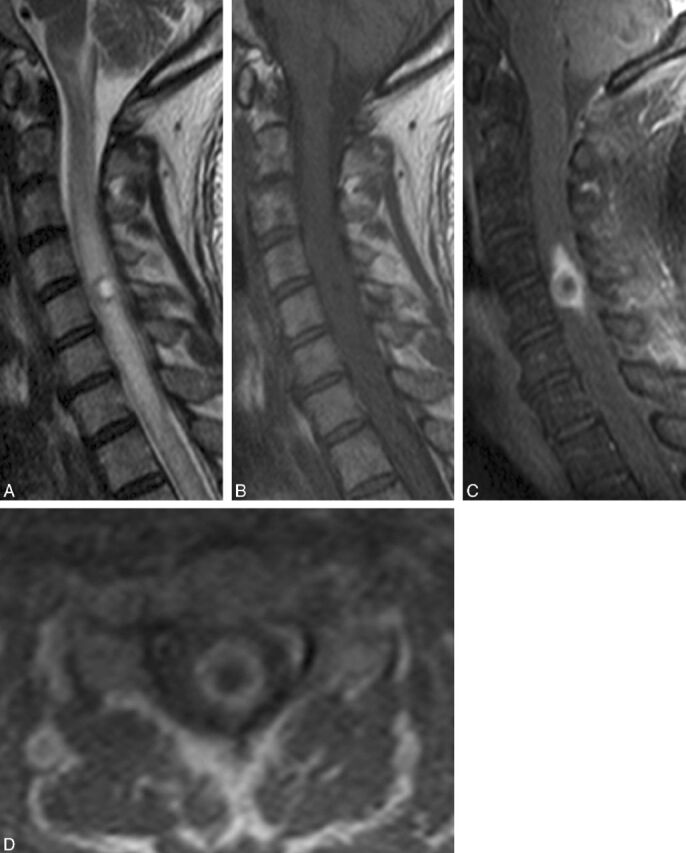
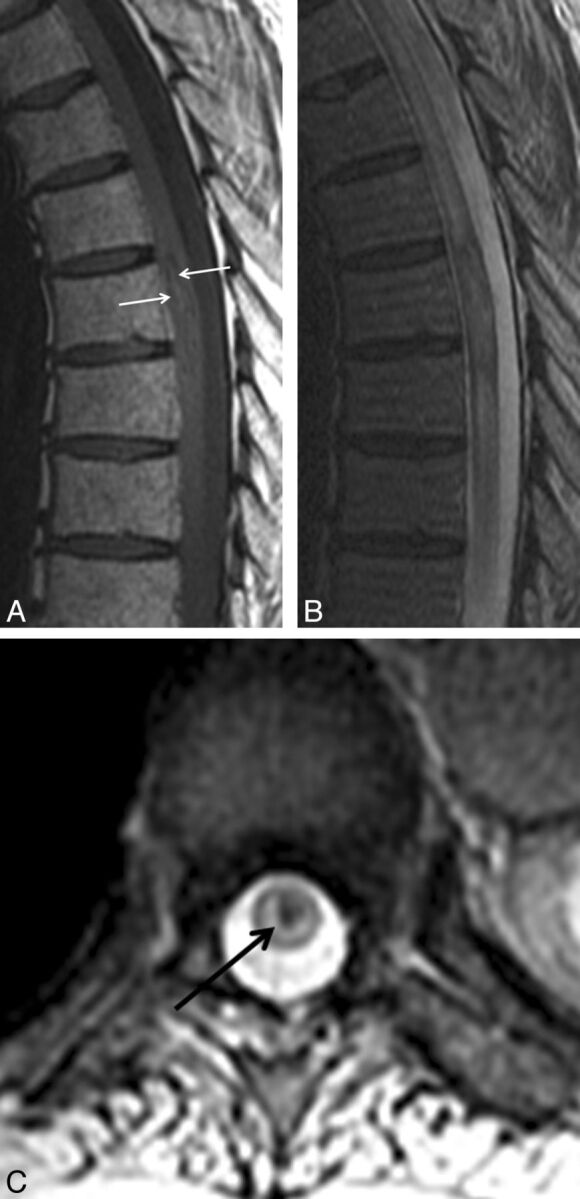
Conclusions: Lack of known primary malignancy or spinal cord symptoms should not discourage consideration of intramedullary spinal cord metastasis. Enhancement and extensive edema for lesion size (often ≥3 segments) are typical for intramedullary spinal cord metastasis. Presence of cystic change/hemorrhage makes intramedullary spinal cord metastasis unlikely. Evidence for other CNS or spinal (non-spinal cord) metastases and the primary tumor/non-CNS metastases are common. The prevalence of other CNS or spinal (non-spinal cord) metastases in those with multiple intramedullary spinal cord metastases is especially high.
Figures

Similar articles
-
Intramedullary spinal cord metastases: prognostic value of MRI and clinical features from a 13-year institutional case series.AJNR Am J Neuroradiol. 2015 Mar;36(3):587-93. doi: 10.3174/ajnr.A4160. Epub 2014 Nov 13. AJNR Am J Neuroradiol. 2015. PMID: 25395656 Free PMC article.
-
Intramedullary spinal cord metastases: visibility on PET and correlation with MRI features.AJNR Am J Neuroradiol. 2014 Jan;35(1):196-201. doi: 10.3174/ajnr.A3618. Epub 2013 Jul 25. AJNR Am J Neuroradiol. 2014. PMID: 23886743 Free PMC article.
-
Intramedullary Spinal Cord Metastasis from Primary Lung Neuroendocrine Carcinoma: A Case Report and Operative Video.World Neurosurg. 2021 Jan;145:426-431. doi: 10.1016/j.wneu.2020.08.103. Epub 2020 Aug 20. World Neurosurg. 2021. PMID: 32827737
-
Intramedullary spinal cord metastasis of lung adenocarcinoma presenting as Brown-Sequard syndrome.Surg Neurol. 2004 Jan;61(1):72-6. doi: 10.1016/s0090-3019(03)00298-2. Surg Neurol. 2004. PMID: 14706385 Review.
-
Intramedullary spinal cord metastasis as a first manifestation of a renal cell carcinoma: report of a case and review of the literature.Clin Neurol Neurosurg. 2000 Dec;102(4):249-254. doi: 10.1016/s0303-8467(00)00106-2. Clin Neurol Neurosurg. 2000. PMID: 11154816 Review.
Cited by
-
Metastatic Complications of Cancer Involving the Central and Peripheral Nervous Systems.Neurol Clin. 2018 Aug;36(3):579-598. doi: 10.1016/j.ncl.2018.04.011. Epub 2018 Jun 15. Neurol Clin. 2018. PMID: 30072072 Free PMC article. Review.
-
Intramedullary spinal cord metastasis in malignancies: an institutional analysis and review.Onco Targets Ther. 2019 Jun 21;12:4741-4753. doi: 10.2147/OTT.S193235. eCollection 2019. Onco Targets Ther. 2019. PMID: 31417275 Free PMC article.
-
Intramedullary spinal cord metastasis from laryngeal carcinoma: case report and review of literature.Pan Afr Med J. 2017 Mar 30;26:189. doi: 10.11604/pamj.2017.26.189.11507. eCollection 2017. Pan Afr Med J. 2017. PMID: 28674582 Free PMC article. Review.
-
Neurologic pathologies of the vertebral spine.Skeletal Radiol. 2024 Mar;53(3):419-436. doi: 10.1007/s00256-023-04428-y. Epub 2023 Aug 17. Skeletal Radiol. 2024. PMID: 37589755 Review.
-
Longitudinally extensive transverse myelitis as presenting manifestation of small cell carcinoma lung.Oxf Med Case Reports. 2015 Feb 26;2015(2):208-10. doi: 10.1093/omcr/omv011. eCollection 2015 Feb. Oxf Med Case Reports. 2015. PMID: 25988082 Free PMC article.
References
-
- Costigan DA, Winkelman MD. Intramedullary spinal cord metastasis: a clinicopathological study of 13 cases. J Neurosurg 1985;62:227–33 - PubMed
-
- Mut M, Schiff D, Shaffrey ME. Metastasis to nervous system: spinal epidural and intramedullary metastases. J Neurooncol 2005;75:43–56 - PubMed
-
- Connolly ES, Jr, Winfree CJ, McCormick PC, et al. . Intramedullary spinal cord metastasis: report of three cases and review of the literature. Surg Neurol 1996;46:329–37 - PubMed
-
- Kalayci M, Cagavi F, Gul S, et al. . Intramedullary spinal cord metastases: diagnosis and treatment–an illustrated review. Acta Neurochir (Wien) 2004;146:1347–54 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical