

Intramedullary spinal cord metastases: MRI and relevant clinical features from a 13-year institutional case series
- PMID: 23620071
- PMCID: PMC7965414
- DOI: 10.3174/ajnr.A3526
Intramedullary spinal cord metastases: MRI and relevant clinical features from a 13-year institutional case series
Abstract
Background and purpose: Because intramedullary spinal cord metastasis is often a difficult diagnosis to make, our purpose was to perform a systematic review of the MR imaging and relevant baseline clinical features of intramedullary spinal cord metastases in a large series.
Materials and methods: Consecutive patients with intramedullary spinal cord metastasis with available pretreatment digital MR imaging examinations were identified. The MR imaging examination(s) for each patient was reviewed by 2 neuroradiologists for various imaging characteristics. Relevant clinical data were obtained.
Results: Forty-nine patients had 70 intramedullary spinal cord metastases, with 10 (20%) having multiple intramedullary spinal cord metastases; 8% (4/49) were asymptomatic. Primary tumor diagnosis was preceded by intramedullary spinal cord metastasis presentation in 20% (10/49) and by intramedullary spinal cord metastasis diagnosis in 10% (5/49); 98% (63/64) of intramedullary spinal cord metastases enhanced. Cord edema was extensive: mean, 4.5 segments, 3.6-fold larger than enhancing lesion, and ≥3 segments in 54% (37/69). Intratumoral cystic change was seen in 3% (2/70) and hemorrhage in 1% (1/70); 59% (29/49) of reference MR imaging examinations displayed other CNS or spinal (non-spinal cord) metastases, and 59% (29/49) exhibited the primary tumor/non-CNS metastases, with 88% (43/49) displaying ≥1 finding and 31% (15/49) displaying both findings. Patients with solitary intramedullary spinal cord metastasis were less likely than those with multiple intramedullary spinal cord metastases to have other CNS or spinal (non-spinal cord) metastases on the reference MR imaging (20/39 [51%] versus 9/10 [90%], respectively; P = .0263).
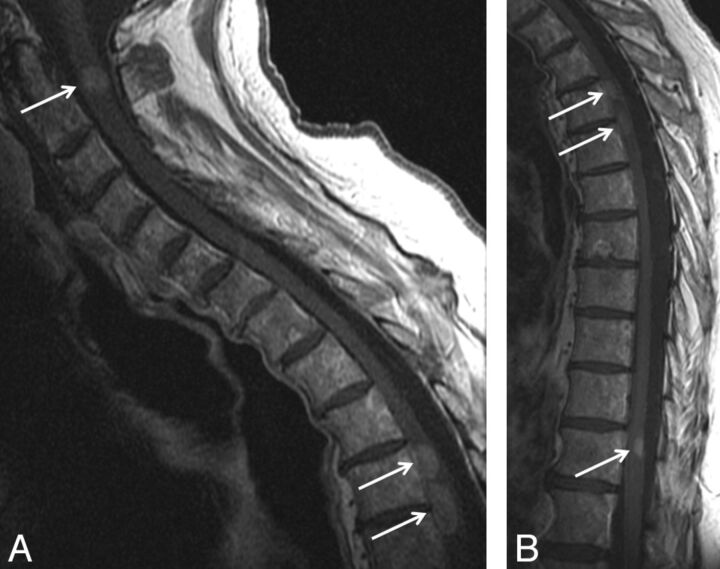
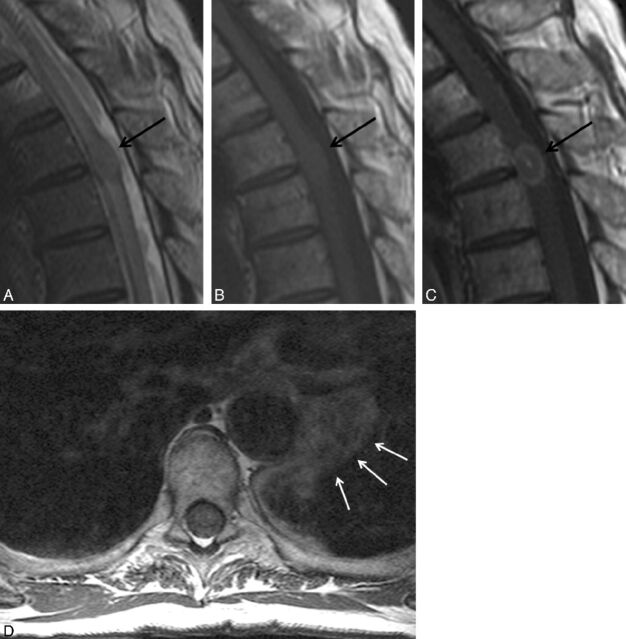
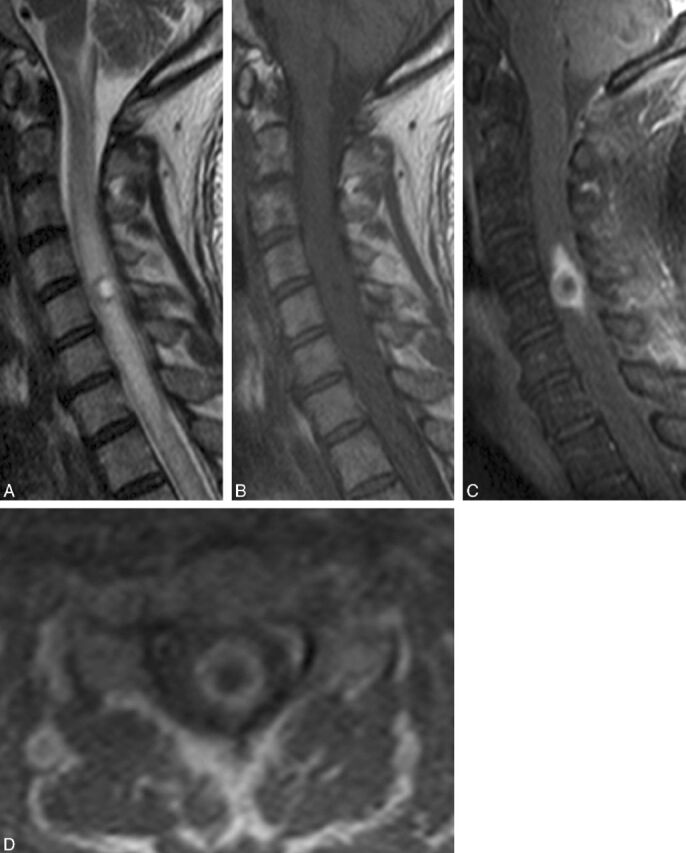
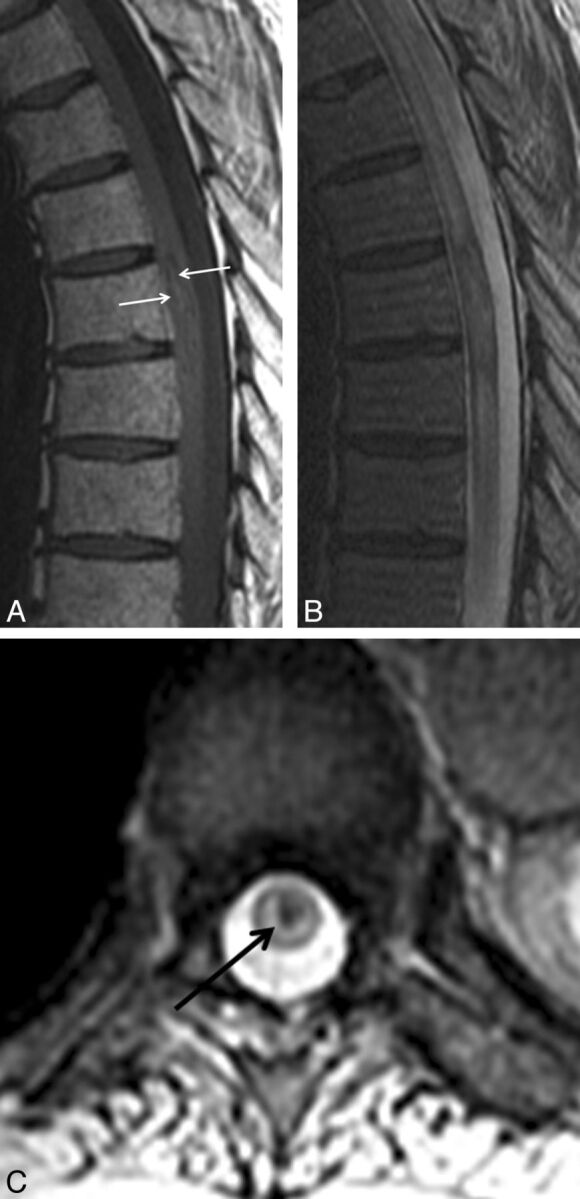
Conclusions: Lack of known primary malignancy or spinal cord symptoms should not discourage consideration of intramedullary spinal cord metastasis. Enhancement and extensive edema for lesion size (often ≥3 segments) are typical for intramedullary spinal cord metastasis. Presence of cystic change/hemorrhage makes intramedullary spinal cord metastasis unlikely. Evidence for other CNS or spinal (non-spinal cord) metastases and the primary tumor/non-CNS metastases are common. The prevalence of other CNS or spinal (non-spinal cord) metastases in those with multiple intramedullary spinal cord metastases is especially high.
Figures

References
-
- Costigan DA, Winkelman MD. Intramedullary spinal cord metastasis: a clinicopathological study of 13 cases. J Neurosurg 1985;62:227–33 - PubMed
-
- Mut M, Schiff D, Shaffrey ME. Metastasis to nervous system: spinal epidural and intramedullary metastases. J Neurooncol 2005;75:43–56 - PubMed
-
- Connolly ES, Jr, Winfree CJ, McCormick PC, et al. Intramedullary spinal cord metastasis: report of three cases and review of the literature. Surg Neurol 1996;46:329–37 - PubMed
-
- Kalayci M, Cagavi F, Gul S, et al. Intramedullary spinal cord metastases: diagnosis and treatment–an illustrated review. Acta Neurochir (Wien) 2004;146:1347–54 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical