

4D digital subtraction angiography: implementation and demonstration of feasibility
- PMID: 23620072
- PMCID: PMC7965425
- DOI: 10.3174/ajnr.A3529
4D digital subtraction angiography: implementation and demonstration of feasibility
Abstract
Background and purpose: Conventional 3D-DSA volumes are reconstructed from a series of projections containing temporal information. It was our purpose to develop a technique which would generate fully time-resolved 3D-DSA vascular volumes having better spatial and temporal resolution than that which is available with CT or MR angiography.
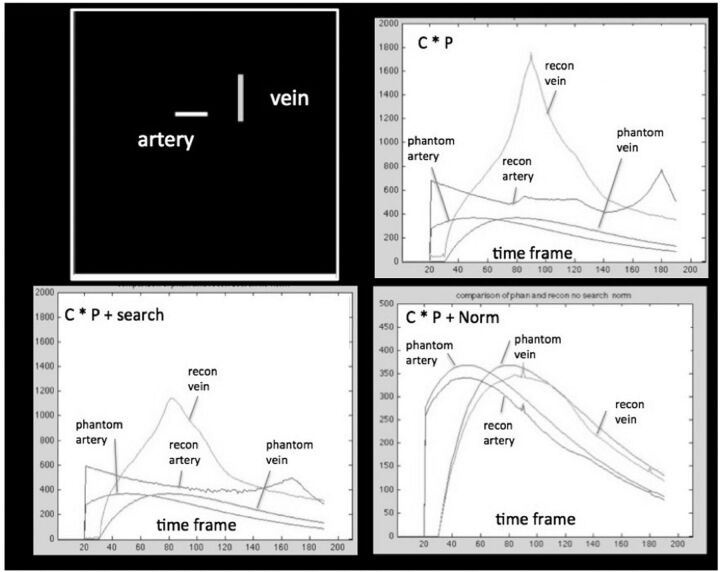
Materials and methods: After a single contrast injection, projections from the mask and fill rotation are subtracted to create a series of vascular projections. With the use of these projections, a conventional conebeam CT reconstruction is generated (conventional 3D-DSA). This is used to constrain the reconstruction of individual 3D temporal volumes, which incorporate temporal information from the acquired projections (4D-DSA).
Results: Typically, 30 temporal volumes per second are generated with the use of currently available flat detector systems, a factor of ∼200 increase over that achievable with the use of multiple gantry rotations. Dynamic displays of the reconstructed volumes are viewable from any angle. Good results have been obtained by using both intra-arterial and intravenous injections.
Conclusions: It is feasible to generate time-resolved 3D-DSA vascular volumes with the use of commercially available flat detector angiographic systems and clinically practical injection protocols. The spatial resolution and signal-to-noise ratio of the time frames are largely determined by that of the conventional 3D-DSA constraining image and not by that of the projections used to generate the 3D reconstruction. The spatial resolution and temporal resolution exceed that of CTA and MRA, and the small vessel contrast is increased relative to that of conventional 2D-DSA due to the use of maximum intensity projections.
Figures






Comment in
-
Four-dimensional digital subtraction angiography: implementation and demonstration of feasibility.World Neurosurg. 2014 Mar-Apr;81(3-4):454-5. doi: 10.1016/j.wneu.2014.01.009. Epub 2014 Jan 20. World Neurosurg. 2014. PMID: 24456826 No abstract available.
References
-
- Mistretta CA, Kruger RA, Houk TL, et al. Computerized fluoroscopy techniques for noninvasive cardiovascular imaging: SPIE. Appl Opt Instr Med 1978;152:65–71
-
- Kruger RA, Mistretta CA, Houk TL, et al. Computerized fluoroscopy in real time for noninvasive visualization of the cardiovascular system: preliminary studies. Radiology 1979;130:49–57 - PubMed
-
- Strother CM, Sackett JF, Crummy AB, et al. Clinical applications of computerized fluoroscopy: the extracranial carotid arteries. Radiology 1980;136:781–83 - PubMed
-
- Ning R, Kruger RA. Computer simulation of image intensifier-based computed tomography detector: vascular application. Med Phys 1988;15:188–92 - PubMed
-
- Ning R, Kruger RA. Image intensifier-based computed tomography volume scanner for angiography. Acad Radiol 1996;3:344–50 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources